Fibermaxxing: What's Real, What's Hype, and How to Actually Add Fiber Without Wrecking Your Gut
"More fiber is not always better. And in some people, adding more fiber actually makes constipation worse."
You added a giant bowl of oats. Then chia seeds. Then a fiber powder. Then a fiber gummy on top of all of it, because a video said this was the move for your hormones and your gut. Now you are bloated, confused, and feeling off, even though your labs are completely normal.
I see this exact picture in clinical conversations every week. Fibermaxxing, the social-media trend of pushing fiber to 40, 50, sometimes 60 grams a day, is not entirely wrong. The premise that most women are under-fibered is correct. The execution is what wrecks people. Fiber is not one nutrient. It is a class of interventions that behave very differently in your body, and matching the right type, the right amount, and the right pace to your specific physiology is what separates benefit from misery.
Below is the framework I wish more women had before they started.
What is fibermaxxing and is it actually safe?
Fibermaxxing is the deliberate practice of pushing fiber intake well above population averages, often to 40 grams a day or more. It is not a clinical protocol. It is a behavioral trend that traces back to one accurate observation: most adults eat about 16 grams of fiber a day on average (Quagliani 2017), against a target of around 25 grams for women. That gap is real.
Where the trend stops being safe is the assumption that more is monotonically better. The dose-response curve for fiber benefit flattens. Tolerance falls if you escalate too fast. And fiber type matters as much as quantity. The same 50-gram-a-day intake that lands fine for one woman will produce three weeks of distension and pain in another, because their starting microbiomes and gut motility are different.
The short answer: fiber is safe and beneficial in the 25 to 35 gram range, built up over weeks. Pushed past that, the tradeoffs start to outweigh the gains for most healthy women, and once you cross 50 grams a day, mineral binding and drug-timing issues become real considerations, especially in women with low ferritin or thyroid medication.
The trend is half right. Build to enough fiber. Do not chase extreme.
How much fiber do you actually need as a woman in your 30s?
For a woman in her 30s, the Adequate Intake established by the Institute of Medicine is 25 grams of fiber a day. The cardiovascular and metabolic benefits captured in dose-response meta-analyses peak in the 25 to 29 gram range and continue with diminishing returns above 30 (Reynolds 2019, Threapleton 2013).
Moving from 15 grams to 25 grams is the most clinically meaningful change you can make. Moving from 30 to 50 grams adds little for most women and adds real digestive cost.
If your current intake is somewhere around 15 grams a day, which is typical, your priority is not 60 grams. Your priority is getting consistent at 25 to 30 from a variety of plants. Trying to hit fibermaxxing levels before you can comfortably hold the 30-gram mark is the most common reason a fiber strategy collapses inside the first month.
Why am I bloated after adding more fiber to my diet?
Bloating after starting fiber is not a sign that fiber does not agree with you. It is a sign of one of three things, and almost every woman I see falls into some combination.
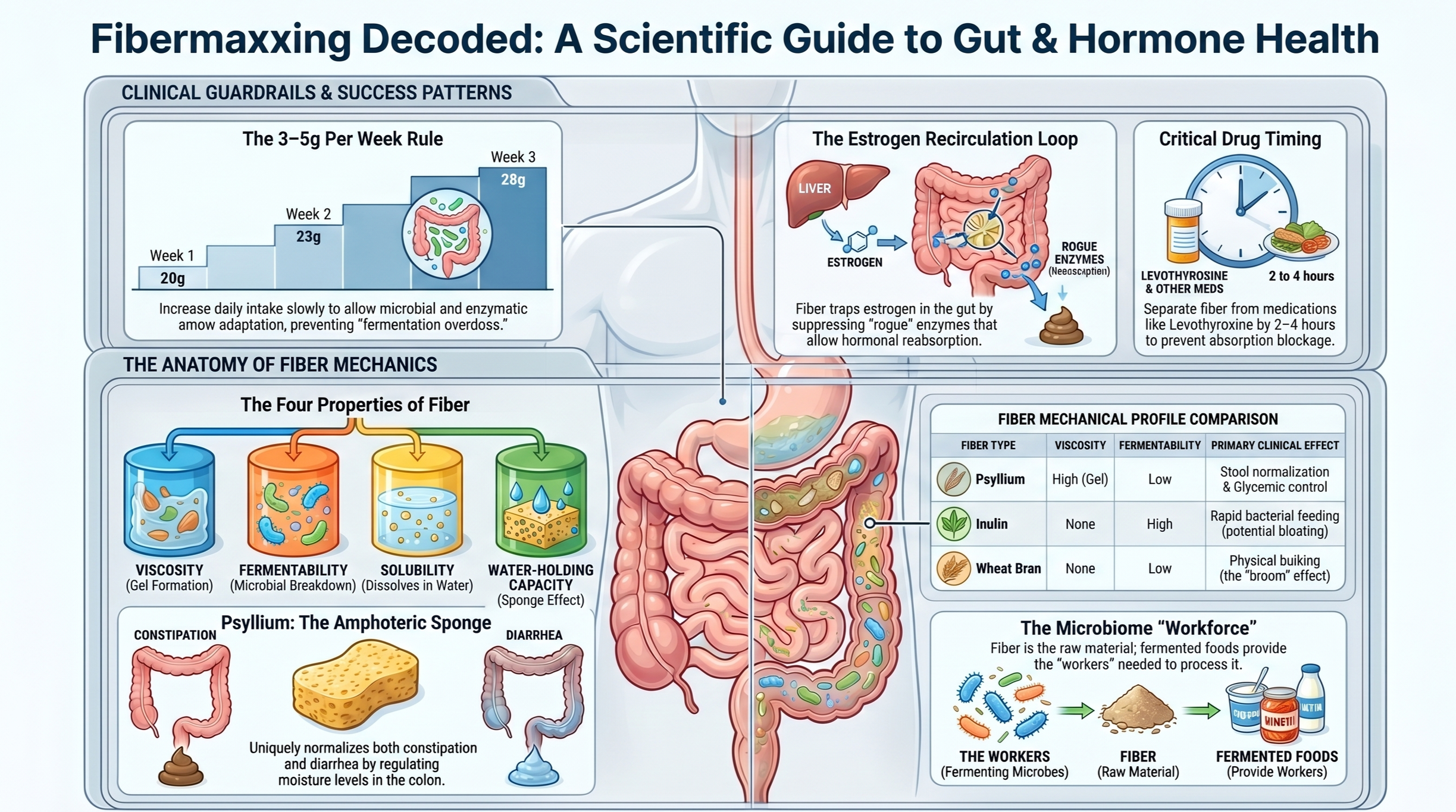
The first is rate of escalation. The clinical standard is the 3-to-5-grams-per-week rule. You add 3 to 5 grams to your total daily fiber each week, not each day. Your enzymes, your gut motility, and your microbial population all need time to adapt, and that takes weeks. If you jump from 15 grams a day to 40 grams over a single weekend, your system cannot keep up. That is the weekend warrior approach to gut health, and it ends in misery.
The second is fiber type mismatch. Highly fermentable fibers like inulin and fructooligosaccharides ferment fast in the colon, producing gas as a normal byproduct. That gas production is physiology, not pathology. If your gut has visceral hypersensitivity, which is when the nervous system in the gut perceives normal stretching as pain, you will feel that gas as severe distension and pain at volumes another person would not notice. Many women in this category get told they have small intestinal bacterial overgrowth (SIBO) when what they actually have is a perfectly normal amount of fermentation in a sensitive gut.
The third is inadequate hydration with bulking fiber. If you increase fiber and do not increase water, the bulk dehydrates in the colon. Hard, dry stool. Slower transit. More straining.
If your bloating is in the first 2 to 4 weeks of an escalation and the rate was reasonable, give it time. If it is severe, you have escalated too fast, mismatched the fiber type, or shorted yourself on water. The fix is mechanical, not diagnostic.
Can too much fiber hurt your gut?
Fiber is one of the few foods that the gut also actively needs. Mouse work by Desai and colleagues showed that when the microbiome is starved of fiber, it begins to eat away at the colonic mucus barrier, which is the protective lining of the gut, and this increases susceptibility to pathogens (Desai 2016). Fiber is structural. You need it.
That said, there is a threshold where fiber stops being protective and starts being a mechanical irritant. At intakes above roughly 50 grams a day, especially in women on low-calorie or restrictive diets, mineral binding becomes a real consideration. Phytic acid in fiber-rich plants binds non-heme iron and zinc and reduces their bioavailability. For an iron-replete woman, this is rarely meaningful. For a woman with menorrhagia, low ferritin, or known iron-deficiency anemia, very-high-fiber intake can compound a negative balance (Hurrell 2010).
The other way fiber hurts is mechanical. If you stack bulking fiber on top of a slow-transit colon or a pelvic floor that does not coordinate properly, more fiber becomes more cars in a traffic jam. That section gets its own discussion later in this post.
What's the difference between soluble and insoluble fiber, and which do you need?
The soluble-versus-insoluble framework you learned is mostly wrong, or at least incomplete. Solubility just means whether the fiber dissolves in water in a laboratory beaker. That tells you very little about how a fiber will behave inside an acidic, enzyme-rich, bacterially populated human gut.
There are four properties that actually drive what a fiber does (McRorie & McKeown 2017):
Solubility. Whether it dissolves in water. Useful as a label, weakest predictor of clinical effect.
Viscosity. Whether it forms a gel when it meets water. This is what makes oat porridge thick and chia seeds turn into pudding overnight. Viscous fibers slow gastric emptying, blunt blood-sugar spikes, and bind bile acids to lower LDL cholesterol.
Fermentability. How fast your gut bacteria can break it down. Highly fermentable fibers feed your microbes and produce short-chain fatty acids, which are the molecules your gut bacteria make from fiber and which fuel the cells of the colon. Highly fermentable fibers also produce the most gas.
Water-holding capacity. Whether the fiber traps water and carries it through the colon. Coarse fibers add about 3 grams of stool weight per gram of fiber consumed.
Once you think in these four properties, every fiber on the market sorts cleanly into a category, and you can predict how your gut will respond.
Inulin (the fiber added to most low-carb processed foods) is non-viscous and highly fermentable. It produces gas. Wheat bran is non-viscous and poorly fermented; it acts as physical bulk. Psyllium is gel-forming and non-fermented, which is why it is in its own category and gets its own section below.
You are not picking one type. You are building a composite from a variety of plants that hits all four properties.
Do fiber gummies actually count as real fiber?
Yes, by the regulatory definition. The FDA allows isolated polysaccharides, which are long-chain carbohydrates, to be labeled as dietary fiber if they meet certain criteria. So a gummy with 3 to 5 grams of chicory root inulin or polydextrose is real fiber on the nutrition label.
What gummies are not is a substitute for whole-food fiber. When you eat an apple, the fiber is bound up in cellular structure that takes time for your body to break down. Fermentation happens slowly, across the digestive tract, with the polyphenols and minerals from the apple coming along for the ride. When you eat an isolated inulin gummy, you deliver a concentrated, highly fermentable load to your colon all at once with no protective matrix. That is a setup for rapid fermentation and immediate bloating in a sensitive gut.
Gummies can be a useful add-on. They cannot be the foundation of a fiber strategy. If your fiber intake comes mostly from supplements while your diet stays low in plants, you will get a narrow physiologic effect and miss the metabolic and microbiome benefits the population studies are actually measuring (Stephen 2017).
Is psyllium husk really better than a fiber supplement?
Psyllium has the strongest evidence base of any single fiber across constipation, diarrhea, blood sugar, and LDL cholesterol. It is the doctor's "boring" pick that quietly outperforms most of the trendy options. Here is why.
Psyllium is the only common fiber that is simultaneously gel-forming, non-fermented, and amphoteric. Amphoteric means it works for both directions of dysfunction; it helps both constipation and diarrhea.
I know that sounds like a contradiction. The way I explain it to women in clinic is the sponge analogy.
Psyllium is a sponge that holds water through the colon. If your stool is too loose, you have too much water in the colon, and the sponge absorbs the excess and gives the stool form. If your stool is too hard, you have too little water in the colon, and the same sponge carries water into the stool and softens it. It normalizes the environment in either direction.
The data backs this up. In a 2020 head-to-head trial, psyllium was 3.4 times more effective than wheat bran for stool output in patients with chronic idiopathic constipation (McRorie 2020). Coarse wheat bran also helped. Finely ground wheat bran actually decreased stool water content and worsened constipation. The same plant, ground differently, produced opposite clinical effects.
Psyllium also has unusually clean metabolic data. A 2015 meta-analysis showed psyllium lowers fasting blood glucose by approximately 37 mg/dL and HbA1c by approximately 0.97 percentage points in patients being treated for type 2 diabetes (Gibb 2015). Those are reductions worth taking seriously. Notably, the effect was proportional to baseline dysregulation; minimal in healthy adults, modest in pre-diabetes, large in type 2 diabetes. Psyllium is not a glucose supplement for everyone. It is a tool for women managing insulin resistance.
If you are choosing a single fiber supplement, this is the one with the most evidence behind it.
How fast can you increase fiber without bloating?
The 3-to-5-grams-per-week rule. That is the answer.
If you currently eat 15 grams a day, aim for 18 to 20 next week, 21 to 25 the week after, and continue building until you settle in the 25 to 35 gram range. Your gut microbes need time to expand the populations that ferment the fiber you are eating. Adaptation happens in weeks, not hours. Respect the timeline.
Hydration belongs in the same conversation. Fiber works partly by holding water in the gut. If you increase fiber and not water, the bulk dehydrates and the colon slows. As a rough rule, every gram of fiber you add asks for a small bump in water intake. The exact volume matters less than the principle.
Distribute fiber across meals rather than front-loading at breakfast. A 30-gram bolus produces a higher fermentation peak than the same 30 grams spread across three or four meals.
Why high fiber may not actually fix your microbiome
This is the section the wellness internet does not want to tell you about, and it is the most important one in this post.
In 2021, a Stanford team led by Hannah Wastyk ran what is called the FeFiFo trial. They put participants on either a high-fiber diet or a high-fermented-food diet for 10 weeks and measured what happened to the microbiome and to inflammatory markers (Wastyk 2021).
The counterintuitive result: the high-fiber arm did not increase microbiome diversity on average. Only women who already had high baseline diversity benefited. People with depleted microbiomes, often from past antibiotic use or long stretches of low-fiber eating, did not see their diversity climb.
The high-fermented-food arm did increase diversity broadly and reduced markers of systemic inflammation across participants.
The way I explain this in clinic is the factory analogy.
Your microbiome is a workforce inside a factory. The fiber you eat is the raw material delivered to the floor. If you have a full, well-trained workforce, more raw material means more output. If your workforce has been thinned (by antibiotics, by post-infectious damage, by years of ultra-processed eating), dropping a massive load of raw material into an empty factory just creates a backlog. You produce more gas per gram of fiber, you ferment less efficiently, and you do not get the benefits.
The clinical implication is that for the post-antibiotic non-responder, fermented foods come first. Yogurt with live cultures, kefir, kimchi, sauerkraut, traditional miso. Build the workforce. Then escalate fiber.
If you have a history of multiple antibiotic courses or long-term restrictive eating, and you have been doing high fiber and feeling worse, this is probably you. The answer is not more fiber. The answer is fermented foods first.
Does fibermaxxing help with hormones and estrogen detox?
The phrase "estrogen detox" is marketing. The mechanism underneath it is real, but smaller than the marketing suggests. Here it is in plain language.
Your liver processes used estrogens, packages them into bile, and sends them into your gut to leave the body in stool. That is the plan. The complication is that some of your gut bacteria produce an enzyme called beta-glucuronidase, which can unpack the estrogen from the bile package and make it available for reabsorption back into the bloodstream. The whole loop, liver to bile to gut and partially back, is called the enterohepatic circulation.
Fiber intervenes in two ways. It binds estrogen physically in the gut, keeping it in the lumen so it has to leave the body. And it reduces beta-glucuronidase activity, so fewer of those bile packages get unpacked in the first place.
The data is older than the trend. In 1982, Goldin and colleagues published a study in the New England Journal of Medicine comparing vegetarian women, who ate around 28 grams of fiber a day, to omnivorous women, who ate around 12 (Goldin 1982). The vegetarian women excreted approximately three times more estrogen in stool. Their plasma estrogens were lower as a result.
Wheat bran appears to be specifically effective for this. In a 1991 controlled trial, wheat bran reduced serum estrone and estradiol in premenopausal women, while oat and corn brans did not (Rose 1991).
Two clinically relevant downstream signals. A 2020 meta-analysis showed about 8 percent lower breast cancer risk in women with higher fiber intake, holding in both premenopausal and postmenopausal cohorts (Farvid 2020). And women with PCOS habitually eat less fiber than controls, which matters because the underlying insulin resistance that drives PCOS is fiber-responsive (Leung 2022).
So the mechanism is real. The magnitude is modest. We are talking about a 10 to 20 percent reduction in plasma estrogens at clinically achievable intakes, an 8 percent lifetime risk reduction for breast cancer in pooled data, and meaningful but not dramatic changes in PCOS markers. This is daily-maintenance physiology, not a detox cleanse. You cannot eat 60 grams of fiber on a Sunday and expect your hormones balanced by Monday morning. What you can do is set a sustained pattern that supports the loop.
Why does fiber cause constipation for some people instead of helping?
Fiber-induced constipation is a real clinical phenomenon and it usually traces to one of three things.
The wrong fiber type. Highly fermentable, non-viscous fibers (inulin, fructooligosaccharides, wheat dextrin) do not provide a meaningful laxative effect. They feed microbes but do not move stool. Finely ground wheat bran, despite being on every "high-fiber" cereal box, can actually decrease stool water content and worsen constipation (McRorie 2020). If you are constipated and you have been adding gummies and fiber-fortified bars, you are likely adding dry bulk without water-holding capacity.
Inadequate hydration with bulking fiber. Fiber that draws water into the colon needs water to draw. If your fluid intake has not increased alongside your fiber, you are creating dense, dehydrated bulk that the colon cannot move easily.
A motility or pelvic-floor problem fiber cannot fix. If you have slow-transit constipation or pelvic floor dyssynergia, which is when the muscles of the pelvic floor contract instead of relax during a bowel movement, more fiber will not solve the problem. It will pile bulk behind a locked door. This is one of the most under-diagnosed reasons women get told to "eat more fiber" indefinitely without ever improving.
There is also a medication-timing issue worth flagging here, even though it is technically a different mechanism. Soluble viscous fiber and bulking fiber can reduce absorption of levothyroxine, the medication used to treat hypothyroidism, when taken at the same time. In a clinical study of hypothyroid patients, fiber-enriched diets significantly decreased the bioavailability of levothyroxine and required dose adjustment (Liel 1996). The fix is timing: separate fiber intake from your levothyroxine dose by at least 2 to 4 hours. The same caution, smaller in magnitude, applies to metformin and certain statins. If you started a high-fiber breakfast and your TSH drifted at your next labs, talk to your prescribing clinician about timing rather than dose.
When more fiber is the wrong answer
Some patterns will not respond to more fiber, no matter how perfectly you titrate. I want to name them so you do not waste months trying.
The first is paradoxical fiber-induced constipation, which I covered above. If bulking fiber is making things worse, less fiber and more water (with a switch to a viscous gel-forming fiber like psyllium) is usually the right move (Ho 2012).
The second is pelvic floor dyssynergia. The muscles of the pelvic floor are supposed to relax during a bowel movement. In dyssynergia, they contract. Adding fiber to a system that physically cannot coordinate an exit just builds a bigger blockage behind a locked door. Dietary fiber does not fix muscle coordination problems. This is the population that benefits from anorectal manometry-guided biofeedback therapy, not nutrition counseling.
The third is the post-antibiotic, low-diversity microbiome non-responder. Discussed above. Fermented foods first.
The fourth is a pattern I want to name carefully and briefly. Sometimes fibermaxxing becomes a vehicle for caloric restriction. The bulk creates a feeling of fullness that lets the person avoid eating adequate calories. The gut symptoms can mimic the other failure modes, but the root cause is psychological, not digestive. If this resonates, the work is not gut work. The work is care.
If you have been doing fiber correctly for 4 to 6 weeks, with the right type, the right pace, and adequate water, and it is still not working, that is data. The next move is evaluation, not more fiber.
Five principles to take with you
If I distilled this whole conversation to five principles, here is what I would give you.
Aim for 25 to 35 grams of fiber a day, from a variety of plants. Most of the cardiometabolic benefit captured in the meta-analyses sits here. You do not need to chase 60.
Build 3 to 5 grams more per week, not per day. The microbiome adapts in weeks. Respect the timeline.
Prefer whole foods over gummies. Use psyllium for specific situations. Constipation, glycemic control, LDL management.
Mind your drug timing. If you are on levothyroxine, separate it from your fiber by at least 2 to 4 hours.
If fiber is not working at 4 to 6 weeks, that is data. The answer is not more fiber. The answer is evaluation. Pelvic floor. Slow transit. Microbiome history. Eating patterns.
Closing
Fiber is not one nutrient. It is a class of interventions that behave very differently in the gut depending on how viscous it is, how fermentable it is, how it holds water, and what kind of microbiome you bring to it. The whole "eat more fiber" advice you have been given for 20 years is not wrong. It is just incomplete. Matching the right type to your physiology, at the right pace, on a gut that is prepared for it, is what separates benefit from iatrogenic bloating, which is bloating caused by the intervention itself.
I did not cover everything here. Cycle-phased fiber dosing (the idea that your fiber tolerance shifts across your menstrual cycle) is a hypothesis I think is worth watching. Fiber strategy on GLP-1 receptor agonists is a real clinical question with almost no trial data behind it yet. Both are worth their own posts. Let me know in the comments if you would be interested in learning more about these topics!
If you take one thing from this, take this. More fiber is not always better. The right fiber, in the right amount, at the right pace, on a gut that is prepared for it. That is what changes things.
Disclaimer
This content is for educational purposes only and is not intended to diagnose, treat, or replace individualized medical care. Please consult your physician or qualified healthcare provider before making changes to your health, especially if you have a medical condition or are taking medications.
References
Reynolds, A., Mann, J., Cummings, J., Winter, N., Mete, E., & Te Morenga, L. (2019). Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. The Lancet, 393(10170), 434-445. PMID: 30638909.
O'Keefe, S. J. D. (2019). The association between dietary fibre deficiency and high-income lifestyle-associated diseases: Burkitt's hypothesis revisited. The Lancet Gastroenterology & Hepatology, 4(12), 984-996. PMID: 31696832.
Quagliani, D., & Felt-Gunderson, P. (2017). Closing America's fiber intake gap: Communication strategies from a food and fiber summit. American Journal of Lifestyle Medicine, 11(1), 80-85. PMID: 30202317.
Slavin, J. (2013). Fiber and prebiotics: Mechanisms and health benefits. Nutrients, 5(4), 1417-1435. PMID: 23609775.
Koh, A., De Vadder, F., Kovatcheva-Datchary, P., & Bäckhed, F. (2016). From dietary fiber to host physiology: Short-chain fatty acids as key bacterial metabolites. Cell, 165(6), 1332-1345. PMID: 27259147.
Desai, M. S., Seekatz, A. M., Koropatkin, N. M., Kamada, N., Hickey, C. A., Wolter, M., Pudlo, N. A., Kitamoto, S., Terrapon, N., Muller, A., Young, V. B., Henrissat, B., Wilmes, P., Stappenbeck, T. S., Núñez, G., & Martens, E. C. (2016). A dietary fiber-deprived gut microbiota degrades the colonic mucus barrier and enhances pathogen susceptibility. Cell, 167(5), 1339-1353.e21. PMID: 27863247.
Makki, K., Deehan, E. C., Walter, J., & Bäckhed, F. (2018). The impact of dietary fiber on gut microbiota in host health and disease. Cell Host & Microbe, 23(6), 705-715. PMID: 29902436.
Threapleton, D. E., Greenwood, D. C., Evans, C. E. L., Cleghorn, C. L., Nykjaer, C., Woodhead, C., Cade, J. E., Gale, C. P., & Burley, V. J. (2013). Dietary fibre intake and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ, 347, f6879. PMID: 24355537.
McRorie, J. W., Jr., & McKeown, N. M. (2017). Understanding the physics of functional fibers in the gastrointestinal tract: An evidence-based approach to resolving enduring misconceptions about insoluble and soluble fiber. Journal of the Academy of Nutrition and Dietetics, 117(2), 251-264. PMID: 27863994.
Halmos, E. P., Power, V. A., Shepherd, S. J., Gibson, P. R., & Muir, J. G. (2014). A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology, 146(1), 67-75.e5. PMID: 24076059.
Ford, A. C., Moayyedi, P., Lacy, B. E., Lembo, A. J., Saito, Y. A., Schiller, L. R., Soffer, E. E., Spiegel, B. M. R., & Quigley, E. M. M. (2014). American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. American Journal of Gastroenterology, 109(Suppl 1), S2-S26. PMID: 25091148.
Ho, K. S., Tan, C. Y. M., Mohd Daud, M. A., & Seow-Choen, F. (2012). Stopping or reducing dietary fiber intake reduces constipation and its associated symptoms. World Journal of Gastroenterology, 18(33), 4593-4596. PMID: 22969234.
Stephen, A. M., Champ, M. M.-J., Cloran, S. J., Fleith, M., van Lieshout, L., Mejborn, H., & Burley, V. J. (2017). Dietary fibre in Europe: Current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutrition Research Reviews, 30(2), 149-190. PMID: 28676135.
McRorie, J. W., Jr. (2015). Evidence-based approach to fiber supplements and clinically meaningful health benefits, part 1: What to look for and how to recommend an effective fiber therapy. Nutrition Today, 50(2), 82-89. PMID: 25972618.
McRorie, J. W., Jr. (2015). Evidence-based approach to fiber supplements and clinically meaningful health benefits, part 2: What to look for and how to recommend an effective fiber therapy. Nutrition Today, 50(2), 90-97. PMID: 25972619.
Anderson, J. W., Baird, P., Davis, R. H., Jr., Ferreri, S., Knudtson, M., Koraym, A., Waters, V., & Williams, C. L. (2009). Health benefits of dietary fiber. Nutrition Reviews, 67(4), 188-205. PMID: 19335713.
Lambeau, K. V., & McRorie, J. W., Jr. (2017). Fiber supplements and clinically proven health benefits: How to recognize and recommend an effective fiber therapy. Journal of the American Association of Nurse Practitioners, 29(4), 216-223. PMID: 28252255.
Soliman, G. A. (2019). Dietary fiber, atherosclerosis, and cardiovascular disease. Nutrients, 11(5), 1155. PMID: 31126110.
Rose, D. P., Goldman, M., Connolly, J. M., & Strong, L. E. (1991). High-fiber diet reduces serum estrogen concentrations in premenopausal women. American Journal of Clinical Nutrition, 54(3), 520-525. PMID: 1652197.
Goldin, B. R., Woods, M. N., Spiegelman, D. L., Longcope, C., Morrill-LaBrode, A., Dwyer, J. T., Gualtieri, L. J., Hertzmark, E., & Gorbach, S. L. (1994). The effect of dietary fat and fiber on serum estrogen concentrations in premenopausal women under controlled dietary conditions. Cancer, 74(3 Suppl), 1125-1131. PMID: 8039147.
Christodoulides, S., Dimidi, E., Fragkos, K. C., Farmer, A. D., Whelan, K., & Scott, S. M. (2016). Systematic review with meta-analysis: Effect of fibre supplementation on chronic idiopathic constipation in adults. Alimentary Pharmacology & Therapeutics, 44(2), 103-116. PMID: 27170558.
Institute of Medicine, Food and Nutrition Board. (2005). Dietary Reference Intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. National Academies Press.
Lacy, B. E., Pimentel, M., Brenner, D. M., Chey, W. D., Keefer, L. A., Long, M. D., & Moshiree, B. (2021). ACG clinical guideline: Management of irritable bowel syndrome. American Journal of Gastroenterology, 116(1), 17-44. PMID: 33315591.
Gibson, G. R., Hutkins, R., Sanders, M. E., Prescott, S. L., Reimer, R. A., Salminen, S. J., Scott, K., Stanton, C., Swanson, K. S., Cani, P. D., Verbeke, K., & Reid, G. (2017). Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nature Reviews Gastroenterology & Hepatology, 14(8), 491-502. PMID: 28611480.
Holscher, H. D. (2017). Dietary fiber and prebiotics and the gastrointestinal microbiota. Gut Microbes, 8(2), 172-184. PMID: 28165863.
Marlett, J. A., McBurney, M. I., & Slavin, J. L. (2002). Position of the American Dietetic Association: Health implications of dietary fiber. Journal of the American Dietetic Association, 102(7), 993-1000. PMID: 12146567.
Wong, J. M. W., de Souza, R., Kendall, C. W. C., Emam, A., & Jenkins, D. J. A. (2006). Colonic health: Fermentation and short chain fatty acids. Journal of Clinical Gastroenterology, 40(3), 235-243. PMID: 16633129.
Hurrell, R., & Egli, I. (2010). Iron bioavailability and dietary reference values. American Journal of Clinical Nutrition, 91(5), 1461S-1467S. PMID: 20200263.
David, L. A., Maurice, C. F., Carmody, R. N., Gootenberg, D. B., Button, J. E., Wolfe, B. E., Ling, A. V., Devlin, A. S., Varma, Y., Fischbach, M. A., Biddinger, S. B., Dutton, R. J., & Turnbaugh, P. J. (2014). Diet rapidly and reproducibly alters the human gut microbiome. Nature, 505(7484), 559-563. PMID: 24336217.
Deehan, E. C., Yang, C., Perez-Muñoz, M. E., Nguyen, N. K., Cheng, C. C., Triador, L., Zhang, Z., Bakal, J. A., & Walter, J. (2020). Precision microbiome modulation with discrete dietary fiber structures directs short-chain fatty acid production. Cell Host & Microbe, 27(3), 389-404.e6. PMID: 32004499.
Sonnenburg, E. D., & Sonnenburg, J. L. (2014). Starving our microbial self: The deleterious consequences of a diet deficient in microbiota-accessible carbohydrates. Cell Metabolism, 20(5), 779-786. PMID: 25156449.
Veronese, N., Solmi, M., Caruso, M. G., Giannelli, G., Osella, A. R., Evangelou, E., Maggi, S., Fontana, L., Stubbs, B., & Tzoulaki, I. (2018). Dietary fiber and health outcomes: An umbrella review of systematic reviews and meta-analyses. American Journal of Clinical Nutrition, 107(3), 436-444. PMID: 29566200.
Staudacher, H. M., Lomer, M. C. E., Farquharson, F. M., Louis, P., Fava, F., Franciosi, E., Scholz, M., Tuohy, K. M., Lindsay, J. O., Irving, P. M., & Whelan, K. (2017). A diet low in FODMAPs reduces symptoms in patients with irritable bowel syndrome and a probiotic restores Bifidobacterium species: A randomized controlled trial. Gastroenterology, 153(4), 936-947. PMID: 28625832.
Bharucha, A. E., Pemberton, J. H., & Locke, G. R., 3rd. (2013). American Gastroenterological Association technical review on constipation. Gastroenterology, 144(1), 218-238. PMID: 23261065.
Suares, N. C., & Ford, A. C. (2011). Systematic review: The effects of fibre in the management of chronic idiopathic constipation. Alimentary Pharmacology & Therapeutics, 33(8), 895-901. PMID: 21332763.
So, D., Whelan, K., Rossi, M., Morrison, M., Holtmann, G., Kelly, J. T., Shanahan, E. R., Staudacher, H. M., & Campbell, K. L. (2018). Dietary fiber intervention on gut microbiota composition in healthy adults: A systematic review and meta-analysis. American Journal of Clinical Nutrition, 107(6), 965-983. PMID: 29757343.
Wastyk, H. C., Fragiadakis, G. K., Perelman, D., Dahl, W. J., Merrill, B. D., Yu, F. B., Topf, M., Gonzalez, C. G., Van Treuren, W., Han, S., Robinson, J. L., Elias, J. E., Sonnenburg, E. D., Gardner, C. D., & Sonnenburg, J. L. (2021). Gut-microbiota-targeted diets modulate human immune status. Cell, 184(16), 4137-4153.e14. PMID: 34256014.
Gibb, R. D., McRorie, J. W., Jr., Russell, D. A., Hasselblad, V., & D'Alessio, D. A. (2015). Psyllium fiber improves glycemic control proportional to loss of glycemic control: A meta-analysis of data in euglycemic subjects, patients at risk of type 2 diabetes mellitus, and patients being treated for type 2 diabetes mellitus. American Journal of Clinical Nutrition, 102(6), 1604-1614. PMID: 26561625.
Jalanka, J., Major, G., Murray, K., Singh, G., Nowak, A., Kurtz, C., Silos-Santiago, I., Johnston, J. M., de Vos, W. M., & Spiller, R. (2019). The effect of psyllium husk on intestinal microbiota in constipated patients and healthy controls. International Journal of Molecular Sciences, 20(2), 433. PMID: 30669509.
Eswaran, S., Muir, J., & Chey, W. D. (2013). Fiber and functional gastrointestinal disorders. American Journal of Gastroenterology, 108(5), 718-727. PMID: 23545709.
Gibson, G. R., & Roberfroid, M. B. (1995). Dietary modulation of the human colonic microbiota: Introducing the concept of prebiotics. Journal of Nutrition, 125(6), 1401-1412. PMID: 7782892.
Burkitt, D. P. (1971). Epidemiology of cancer of the colon and rectum. Cancer, 28(1), 3-13. PMID: 5165022.
Vandeputte, D., Falony, G., Vieira-Silva, S., Wang, J., Sailer, M., Theis, S., Verbeke, K., & Raes, J. (2017). Prebiotic inulin-type fructans induce specific changes in the human gut microbiota. Gut, 66(11), 1968-1974. PMID: 28213610.
Kaczmarczyk, M. M., Miller, M. J., & Freund, G. G. (2012). The health benefits of dietary fiber: Beyond the usual suspects of type 2 diabetes mellitus, cardiovascular disease and colon cancer. Metabolism, 61(8), 1058-1066. PMID: 22401879.
Barber, T. M., Kabisch, S., Pfeiffer, A. F. H., & Weickert, M. O. (2020). The health benefits of dietary fibre. Nutrients, 12(10), 3209. PMID: 33096647.
Lattimer, J. M., & Haub, M. D. (2010). Effects of dietary fiber and its components on metabolic health. Nutrients, 2(12), 1266-1289. PMID: 22254008.
Goldin, B. R., Adlercreutz, H., Gorbach, S. L., Warram, J. H., Dwyer, J. T., Swenson, L., & Woods, M. N. (1982). Estrogen excretion patterns and plasma levels in vegetarian and omnivorous women. New England Journal of Medicine, 307(25), 1542-1547. PMID: 7144835.
Leung, W. T., Tang, Z., Feng, Y., Guan, H., Huang, Z., & Zhang, W. (2022). Lower fiber consumption in women with polycystic ovary syndrome: A meta-analysis of observational studies. Nutrients, 14(24), 5285. PMID: 36558444.
Farvid, M. S., Spence, N. D., Holmes, M. D., & Barnett, J. B. (2020). Fiber consumption and breast cancer incidence: A systematic review and meta-analysis of prospective studies. Cancer, 126(13), 3061-3075. PMID: 32249416.
McRorie, J. W., Jr., Fahey, G. C., Jr., Gibb, R. D., & Chey, W. D. (2020). Laxative effects of wheat bran and psyllium: Resolving enduring misconceptions about fiber in treatment guidelines for chronic idiopathic constipation. Journal of the American Association of Nurse Practitioners, 32(1), 15-23. PMID: 31764399.
Dhingra, D., Michael, M., Rajput, H., & Patil, R. T. (2012). Dietary fibre in foods: A review. Journal of Food Science and Technology, 49(3), 255-266. PMID: 23729846.