PCOS Has a New Name (PMOS): What Actually Changes for You
If you saw the headlines this week and felt that flicker of “wait, did my diagnosis just change,” you are not alone. The condition you have been calling PCOS (polycystic ovary syndrome) was formally renamed to PMOS (polyendocrine metabolic ovarian syndrome) on May 12, 2026, by a global consensus panel published in The Lancet. The internet immediately split into two camps. One side says the rename is overdue and that ovaries were never the real story. The other side says the timing is dismissive of the people who have been living with this label for years.
I want to give you a third reading, the one I have not seen in the coverage so far. The rename is rigorous and directionally right. It is also clinically incomplete in a way that matters for you specifically. In this post I will walk you through what actually changed, what did not change on Monday morning, why the metabolic framing is mostly correct, where it falls short, and the six questions worth bringing to your next appointment. By the end you will know how to use this without being used by it.
What just changed: the rename from PCOS to PMOS
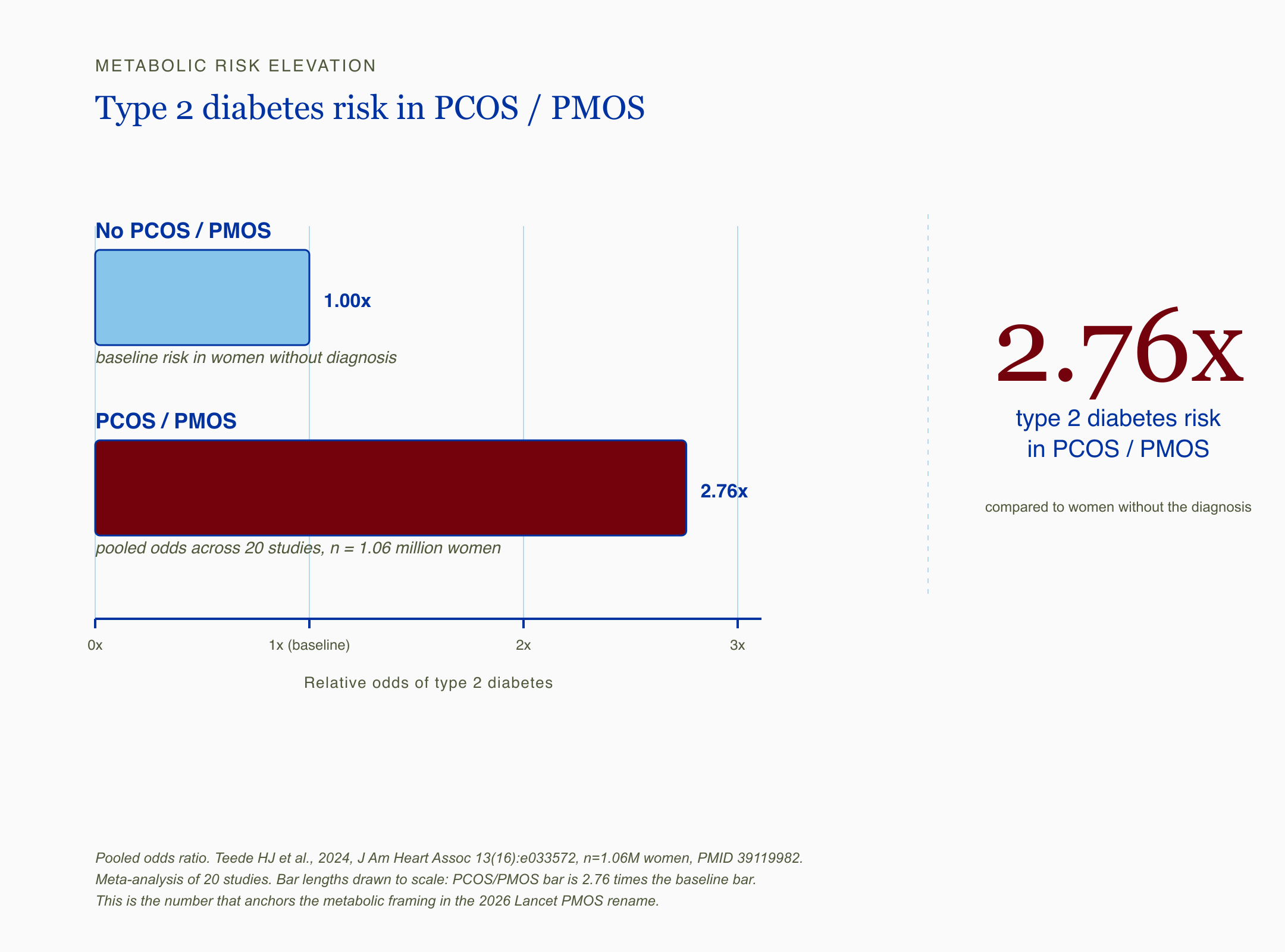
A horizontal bar chart comparing type 2 diabetes risk in PCOS/PMOS versus women without the diagnosis. The PCOS/PMOS bar is 2.76 times longer than the baseline bar, with a large 2.76x callout in crimson on the right.
Before any of the lab talk, I want to acknowledge what most of you are feeling. You have spent years explaining a condition with a name nobody understood, including some of your own doctors. A different name on the chart does not erase that history.
The short answer: The 2026 Lancet consensus paper renamed PCOS to PMOS (polyendocrine metabolic ovarian syndrome) after an eleven-year multi-stakeholder process led by Helena Teede and 56 organizations. The diagnostic criteria did not change. The treatment guidelines did not change. The condition you have is the same one you had on May 11.
The rename reflects three things the field has been saying for over a decade. First, the ovary is not the headline organ. The dominant features are endocrine and metabolic, with ovarian morphology as one piece of the picture, not the lead. Second, the word “cyst” was never accurate. The ultrasound findings are immature follicles, not pathological cysts. Third, the old name kept patients and clinicians fixated on the ovaries while the diabetes risk, the cardiovascular risk, and the liver risk quietly accumulated in the background.
The 2026 Lancet PMOS rename won 86% patient and 71% clinician support across 22,000 global respondents. That is unusually high agreement for a rename of this magnitude. The process was not cavalier.
Bottom line so far: The rename is real. The science it reflects is real. What it changes for you in a 15-minute appointment next month is a separate question, and the honest answer is “less than the headlines suggest.”
Does this change anything for you on Monday morning?
Here is the part that affects you in the actual exam room. The new name does not change your billing codes, your lab requisitions, your insurance authorization, or your treatment plan. Your chart will most likely still say PCOS for the next twelve to thirty-six months while ICD codes and EHR templates catch up.
The short answer: No, not yet. The diagnosis stays the same. The criteria (Rotterdam) stay the same. The first-line treatments (lifestyle change, letrozole for ovulation induction, metformin for metabolic features) stay the same. The label on your chart will be in transition for at least a year, probably longer.
What this means for the woman in front of me is simple. Use whichever name your provider recognizes. The syllables do not matter as much as the questions you ask, and the questions are below. If your doctor says PMOS and means PCOS, you are talking about the same thing. If your doctor has never heard of PMOS yet, that is expected. The transition period the Lancet authors built into the rollout is three years.
One small note. I have seen women I work with arrive at appointments armed with a printed copy of the Lancet paper and a long list of corrections for their doctor. That posture rarely lands well, even when the patient is technically right. The questions in the save card below are designed to do the same intellectual work without the friction.
Bottom line: The name on your chart is in flux. The science of the condition is not. The clinical action is the same on Monday as it was the Friday before.
Why the metabolic framing is mostly right
A four-node circular loop showing how elevated insulin lowers SHBG, raises free testosterone, and worsens insulin resistance, with the cycle perpetuating as the engine of PCOS/PMOS.
I want to start this section the way I would start it if you were sitting across from me with a stack of normal labs and a body that has not felt right in three years. The metabolic framing is not a wellness reframe. It is what the largest data sets have been saying for a decade.
The short answer: The metabolic risk in PCOS/PMOS is substantial and underappreciated. Type 2 diabetes (T2DM, the chronic form of high blood sugar driven by insulin resistance), cardiovascular disease, and non-alcoholic fatty liver (NAFLD, also called MASLD in newer guidelines, where fat accumulates in the liver in someone who does not drink heavily) all run at meaningfully higher rates in this population than in women without the diagnosis.
PCOS, now PMOS, raises type 2 diabetes risk 2.76-fold, per a 2024 AHA meta-analysis of 1.06 million women. That number is from a pooled analysis across twenty studies. It is not a wellness statistic. It is the largest synthesis the cardiology and endocrinology communities have on this question, and it has solid data behind it.
The mechanism most people will not get explained in their appointment runs like this. Insulin resistance (the cells getting deaf to insulin’s signal, so the pancreas has to shout louder) drives elevated insulin, which drives ovarian androgen production (raised levels of male-pattern hormones like testosterone), which suppresses SHBG (sex hormone binding globulin, the protein that ferries sex hormones around the bloodstream), which raises the free testosterone fraction, which produces the hyperandrogenism signs (hair growth in male-pattern locations, acne, hair thinning) you and your dermatologist have been managing for years. The ovary is the visible site. The pancreas is the engine.
This is why the rename matters. PCOS positioned the ovary as the disease. PMOS positions the metabolic system as the engine, with the ovary as one of several end-organs that show the strain. From the perspective of long-term risk reduction, that reframing is correct. Cardiovascular disease and T2DM are the conditions that will most likely take years off the life of an undertreated PCOS patient, not the cysts.
Bottom line: The metabolic story is the right story for most women with this diagnosis, and the rename gets the emphasis right. The number to remember is the 2.76-fold T2DM risk, because it is the number that will most likely move your provider when other framings have not.
The lab most doctors will not run: fasting insulin and HOMA-IR
If you take one thing from this post into your next appointment, take this section. The single most useful test for catching the actual mechanism in this condition is the one most often left off the lab order.
The short answer: HbA1c (the three-month average blood sugar marker conventional medicine relies on for diabetes screening) misses early insulin resistance routinely. Fasting insulin, paired with fasting glucose to calculate HOMA-IR (a simple math formula that estimates insulin resistance from two blood values you already have), catches insulin dysregulation years before HbA1c moves into the abnormal range.
Here is the line I keep coming back to in cases I have reviewed. A 32-year-old with cycles every 60 days, mild adult acne, a normal BMI, and an HbA1c of 5.3 walks out of her appointment with a clean bill of metabolic health. Her fasting insulin, if anyone had ordered it, would have read 19 microIU/mL. That is not metabolic health. That is the pancreas working overtime to keep glucose in the normal range, and it is exactly the pattern PMOS is trying to make visible.
Insulin resistance hits 75% of lean PCOS patients, even when HbA1c reads normal, per a 2022 phenotype review. Three-quarters. In lean women. With normal HbA1c. This is why the metabolic story is not a “weight” story, and why the woman in front of me who has been told her labs are fine often is not fine. The screening tool conventional care is using catches the late stage of this disease, not the early stage.
What this means for you. If you are in this conversation and you have never had a fasting insulin drawn, that is the test worth asking for. It is inexpensive, widely available, and interpretable with a calculator. The HOMA-IR formula is fasting insulin times fasting glucose divided by 405, with a result above roughly 2.0 to 2.5 suggesting insulin resistance depending on the lab and the population. Your provider can run it. They may not order it unless you ask.
I see this consistently in cases I have reviewed. The trials matching HbA1c versus fasting insulin head-to-head in this specific population are smaller than I would like, and the international guidelines still center HbA1c for screening. But the mechanism research is clear, and the lived clinical pattern is clearer. The lab that catches this disease early is the one your appointment is least likely to include.
Bottom line: Ask for fasting insulin. Ask for HOMA-IR. Bring the calculation to your follow-up. The screening test that catches the actual mechanism is the one most often left off.
The phenotype problem: who the metabolic story misses
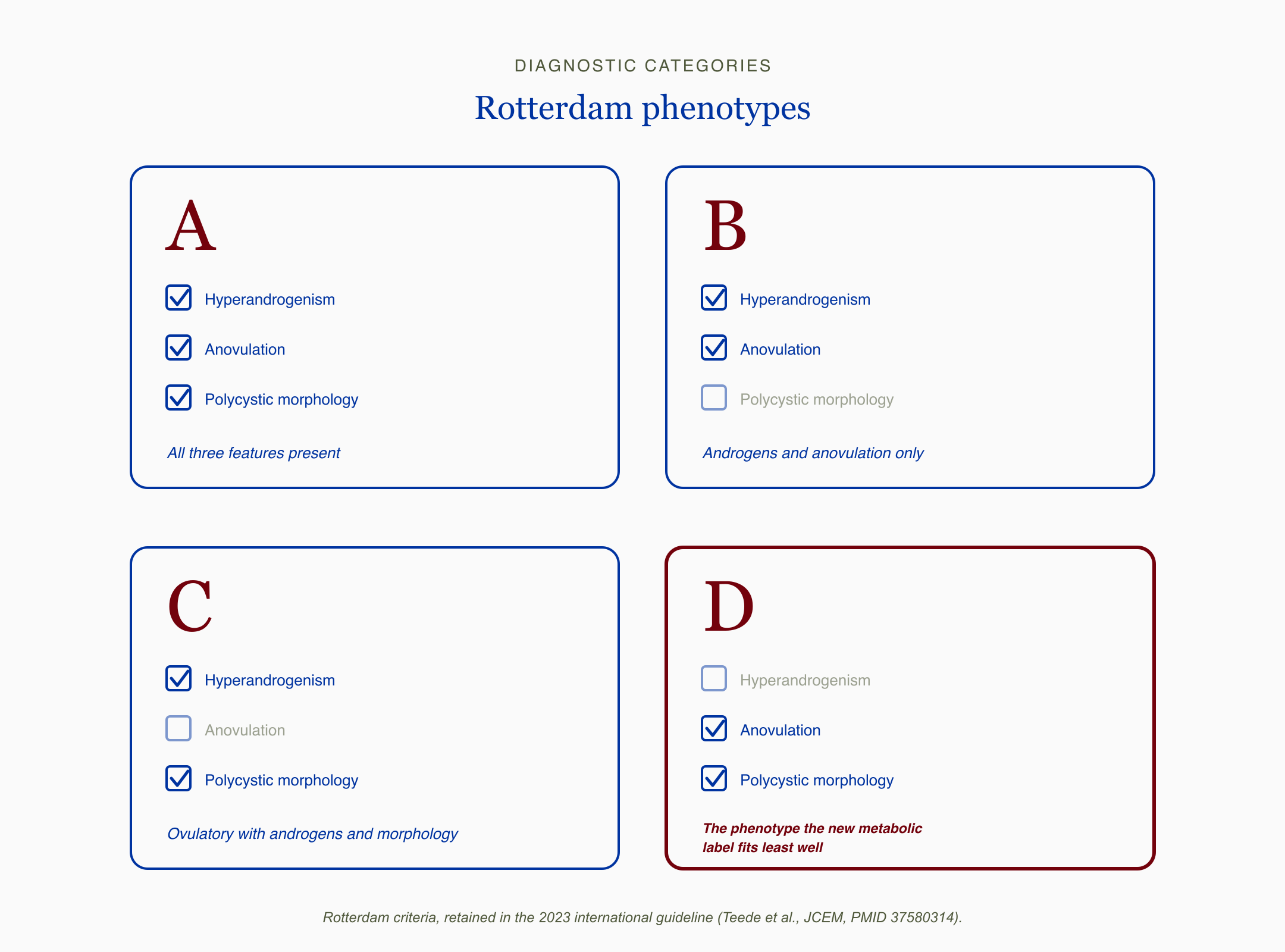
A two-by-two grid of the four Rotterdam phenotypes A, B, C, and D, with checkboxes for hyperandrogenism, anovulation, and polycystic morphology. Phenotype D is highlighted in crimson as the phenotype the new metabolic label fits least well.
I want to slow down here, because this is the section I have not seen anyone else write clearly. If you are a lean woman with irregular cycles and polycystic-appearing ovaries on ultrasound, the new name might make you feel like you no longer belong in this diagnosis. You do. The science is just messier than the headlines.
The short answer: The Rotterdam phenotypes (A, B, C, and D, the four diagnostic categories within PCOS based on which combinations of irregular cycles, high androgens, and polycystic ovarian morphology a patient has) carry meaningfully different metabolic profiles. Phenotype D (the lean, ovulatory-dysfunction-plus-polycystic-morphology pattern without hyperandrogenism) often runs without textbook insulin resistance. The metabolic framing fits A, B, and C cleanly. It fits D the least well.
I have seen women with PCOS whose HbA1c reads 5.4 while fasting insulin runs 18, and conventional care reads that pair as 'fine.
Phenotype A carries both hyperandrogenism and ovulatory dysfunction and polycystic morphology. Phenotype B carries hyperandrogenism and ovulatory dysfunction without the morphology. Phenotype C carries hyperandrogenism with morphology but ovulates. Phenotype D carries ovulatory dysfunction and morphology without hyperandrogenism. Each phenotype has a different metabolic risk profile. Lean phenotype D is the corner of this diagnosis where the metabolic engine often is not the dominant driver, and the patient is not at the same level of T2DM risk as the classic A or B phenotype.
What this means for you. If you are a phenotype D patient (lean, ovulatory dysfunction, polycystic morphology, no hyperandrogenism), the new framing is not wrong, it is just not the whole story for your body. Your concerns may center more on cycle regulation, fertility, and the LH/FSH ratio (luteinizing hormone to follicle-stimulating hormone, two pituitary hormones whose imbalance is a marker in this phenotype) than on insulin and lipids. The first-line treatment is still lifestyle. The pharmacology may diverge.
This is also where the “no doctor I’ve seen seems trained to investigate this properly” comment lands hardest. The conventional provider is being trained on the modal patient, which is phenotype A. The wellness internet is being trained on the modal patient, which is also phenotype A. Phenotype D is the patient both ecosystems treat as an exception when in fact she is one of the four diagnostic categories.
Bottom line: The metabolic framing is right for most patients with this diagnosis. It is not right for all of them. If you are lean and ovulatory with polycystic morphology, ask your provider where you fit in the Rotterdam framework before accepting the metabolic-dominance story as your story.
What the rename does not solve: the screening failure
This is the part that frustrates me the most about the coverage so far. The diagnostic delay in PCOS/PMOS is not a naming problem. It is a screening problem. And a name change does not put fasting insulin on the lab order.
The short answer: Roughly 70% of women with this condition are undiagnosed. Average diagnostic delay runs two to over four years. The average patient sees three or more physicians before getting the diagnosis. A new name does not change any of these structural numbers on its own.
I have read every major piece of coverage on the rename since the Lancet paper dropped. The framing across most of them is “this will help with diagnosis.” That is a claim, not a finding. The Lancet paper itself does not show outcomes data on diagnostic delay because the rename happened four days before this post. The honest answer is that no one knows yet whether PMOS will improve diagnosis, and the structural barriers (10-minute appointments, lab panels that center HbA1c over fasting insulin, ovarian-morphology-first diagnostic mental models in primary care) are exactly the same on May 16 as they were on May 11.
What this means for the woman in front of me is this. Do not wait for the rebrand to filter through to your appointment. The lever that moves your diagnosis forward is the same one it was last year. Ask for the specific tests. Ask which phenotype you match. Ask about cardiovascular risk assessment regardless of your weight or age. Bring the questions, not the syllables.
I want to be precise about my disagreement with the more optimistic framing here. I am not saying the rename is wrong. The Lancet authors and the 56 organizations that participated did real work over more than a decade. The patient survey support of 86% is meaningful. My objection is narrower. The rename was the easy lift compared to the structural changes the field actually needs. A name change cost the consensus panel a lot of meeting hours. Putting fasting insulin on every PCOS/PMOS workup would cost the field a coordinated guideline rewrite and a payer alignment that I have not yet found evidence is being planned.
Bottom line: The rename is a credible first step. It is not the step that ends the diagnostic delay. The work the patient still has to do in the appointment is the same.
What I’d do this week
If you are someone who has been told your ovaries look fine, or your labs are normal, or your cycles are “probably just stress,” the most useful thing you can take into your next appointment is a structured set of questions. Below is the card I would bring.
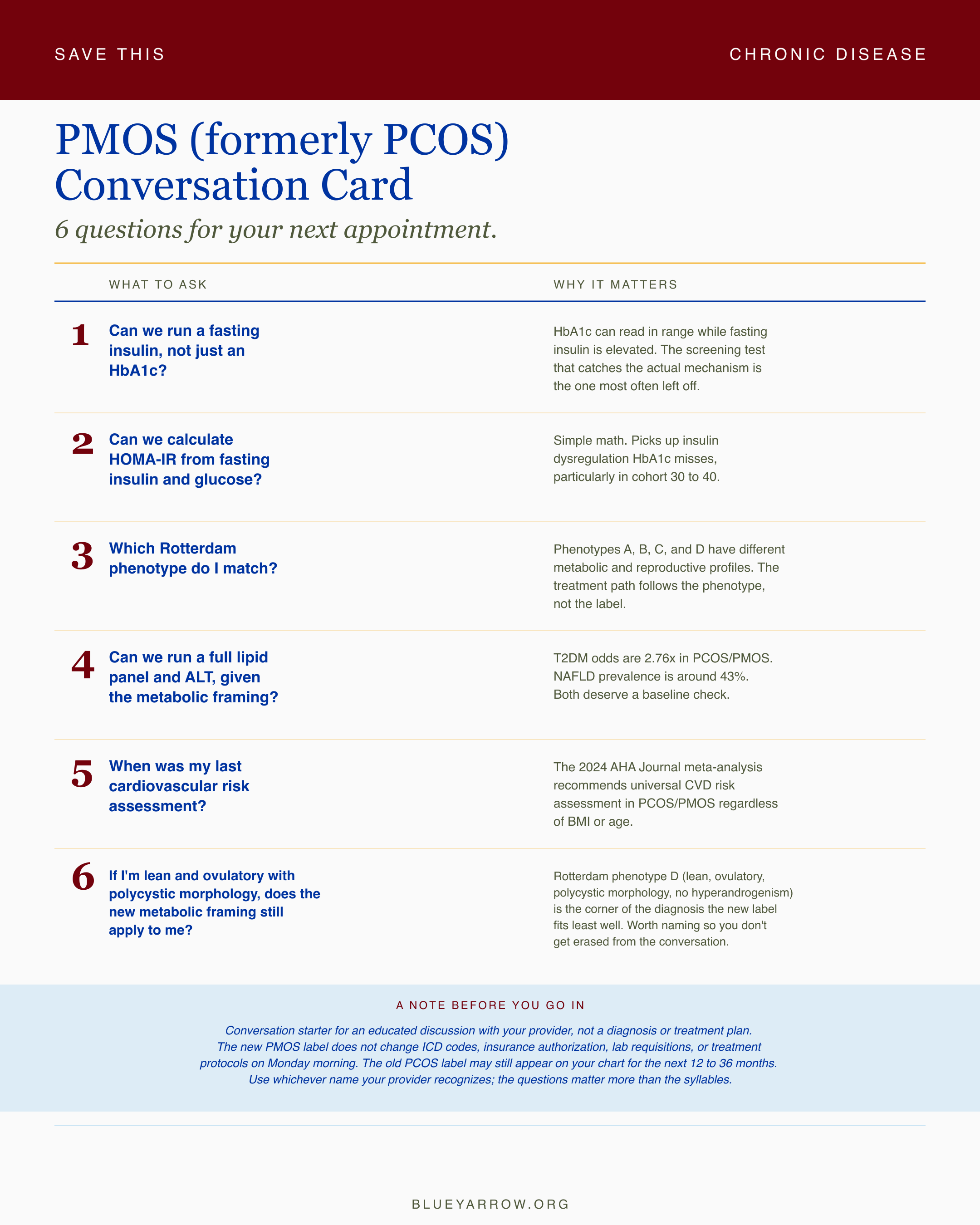
PMOS (formerly PCOS) Conversation Card: 6 questions for your next appointment
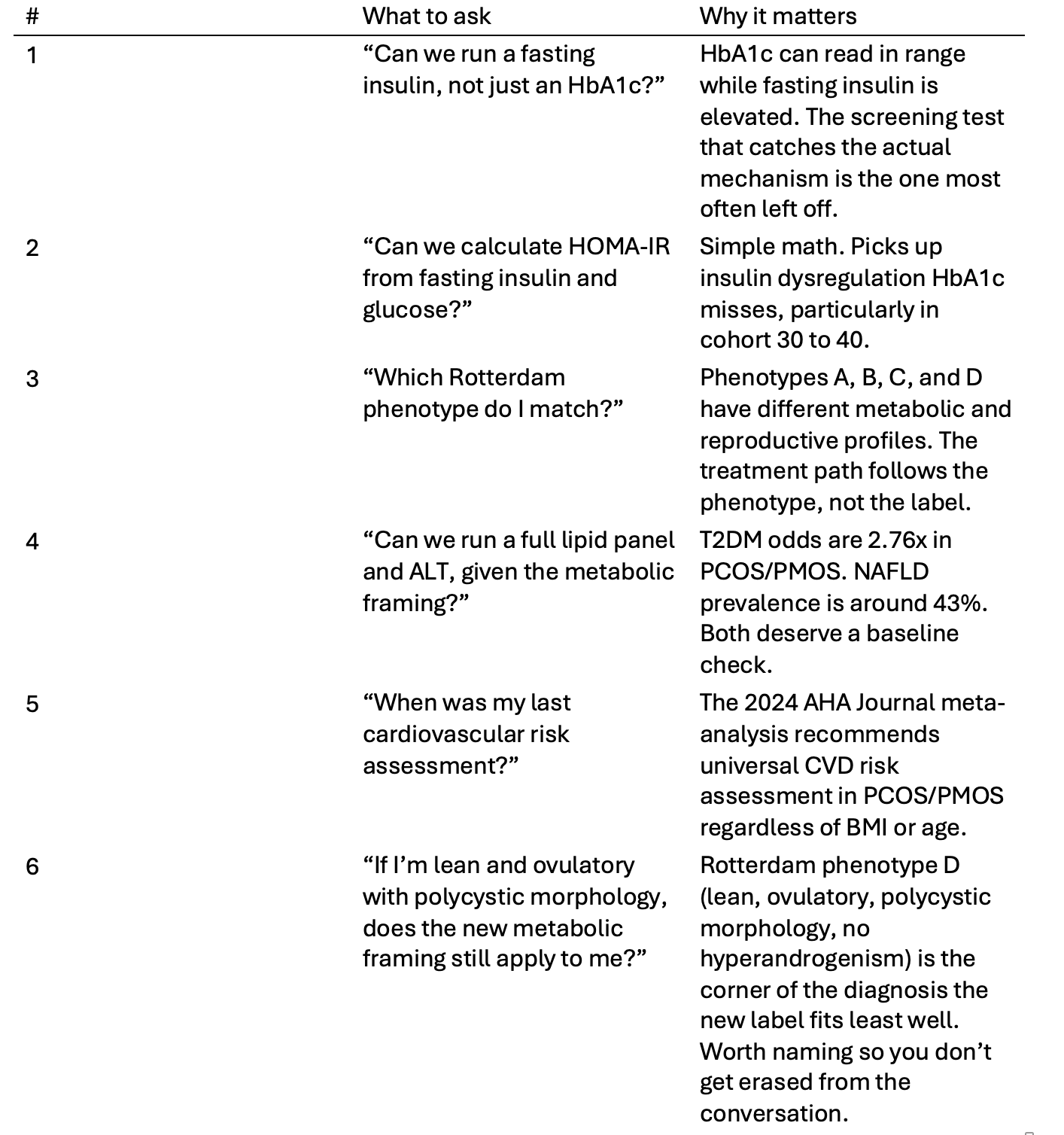
Caveat row: This is a conversation starter for an educated discussion with your provider, not a diagnosis or treatment plan. The new PMOS label does not change ICD codes, insurance authorization, lab requisitions, or treatment protocols on Monday morning. The old PCOS label may still appear on your chart for the next 12 to 36 months. Use whichever name your provider recognizes; the questions matter more than the syllables.
If your provider runs only one of these, make it question one. Fasting insulin is the lever. Everything else builds on it.
Bottom line: Six questions. One appointment. The save-card here is intentionally structured so you can screenshot it, write it in a notebook, or hand it to your provider. The questions matter more than the syllables.
The honest verdict: directionally right, clinically incomplete
I want to land this somewhere truthful rather than tidy. The 2026 Lancet rename is rigorous, well-evidenced, and pointed in the right direction. The metabolic framing is what the largest data sets have been saying for a decade. The patient and clinician support numbers are unusually high. The Lancet authors did the work.
And the rename does not change your lab order. It does not change your insurance authorization. It does not put fasting insulin on the universal PCOS/PMOS workup. It does not address the screening failure that leaves the majority of women in this category undiagnosed. It does not protect phenotype D from being erased by the metabolic-dominance story. None of this makes the rename a mistake. All of it makes the rename insufficient on its own.
If you have been in this diagnosis for years, I think the most useful posture is patience with the language and impatience with the structure. The chart label will catch up. The 10-minute appointment, the HbA1c-first workup, and the ovary-as-headline mental model will catch up more slowly, and only if patients keep asking the questions that move the workup forward.
The work in front of you is the same work it was on May 11. Know your phenotype. Know your fasting insulin. Know your cardiovascular risk. Treat the metabolic engine. Use whatever name your provider knows. Trust the questions more than the syllables.
What would you want to ask your provider that this post did not cover? I read every reply.
Frequently asked questions
Is PMOS the same as PCOS? Yes. PMOS (polyendocrine metabolic ovarian syndrome) and PCOS (polycystic ovary syndrome) describe the same clinical condition. The 2026 Lancet consensus paper renamed it to better reflect the metabolic and endocrine dimensions of the disease. Diagnostic criteria, treatment guidelines, and ICD codes remain unchanged for now.
Do I need a new diagnosis or new lab work after the rename? No. The diagnostic criteria did not change. If you already have a PCOS diagnosis, that diagnosis stands. The rename is a relabeling, not a re-evaluation. New lab work is only indicated if your clinical picture has changed or if foundational tests like fasting insulin were never run on you.
Why did they change the name from PCOS to PMOS? The 2026 Lancet paper, supported by 86% of 14,360 patient respondents and 71% of clinicians across 22,000 total responses, concluded that the old name overemphasized ovarian morphology and underemphasized the metabolic and endocrine drivers. The rename centers the actual disease mechanism rather than its visible ovarian sign.
Does PMOS mean I definitely have insulin resistance? Not necessarily. Insulin resistance affects roughly 75% of lean PCOS patients per the 2022 phenotype review, but Rotterdam phenotype D (lean, ovulatory dysfunction, polycystic morphology, no hyperandrogenism) often runs without textbook insulin resistance. Knowing your phenotype matters more than assuming the metabolic story applies to your specific case.
What is the best test to ask my doctor for if I think I have PMOS? Fasting insulin paired with fasting glucose to calculate HOMA-IR is the highest-yield request. HbA1c, the conventional screening test, can read normal while fasting insulin is elevated. The 2024 AHA meta-analysis of 1.06 million women showed a 2.76-fold elevation in T2DM risk in this population, which makes early insulin dysregulation worth catching before HbA1c moves.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
Teede, H. J., Khomami, M. B., Morman, R., et al. (2026). Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome: a multistep global consensus process. The Lancet. PMID: 42119588. DOI: 10.1016/S0140-6736(26)00717-8.
Teede, H. J., et al. (2024). 2023 International Evidence-Based Polycystic Ovary Syndrome Guideline Update: Insights From a Systematic Review and Meta-Analysis on Elevated Clinical Cardiovascular Disease in Polycystic Ovary Syndrome. Journal of the American Heart Association, 13(16), e033572. PMID: 39119982. DOI: 10.1161/JAHA.123.033572.
Teede, H. J., Tay, C. T., Laven, J., et al. (2023). Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Journal of Clinical Endocrinology & Metabolism, 108(10), 2447-2469. PMID: 37580314.
Lean vs. Obese PCOS Phenotype Authors. (2022). Comparing Lean and Obese PCOS in Different PCOS Phenotypes: Evidence That the Body Weight Is More Important than the Rotterdam Phenotype in Influencing the Metabolic Status. PMC9600591.
Insulin Resistance Mechanism Review Authors. (2025). Insulin resistance in polycystic ovary syndrome phenotypes and the vicious cycle model in its etiology. Scientific Reports.
Markers of Insulin Resistance Review Authors. (2022). Markers of insulin resistance in Polycystic ovary syndrome women: An update. PMC8984569.
NAFLD-PCOS Meta-Analysis Group. (2023). Non-Alcoholic Fatty Liver Disease in Patients with Polycystic Ovary Syndrome: A Systematic Review, Meta-Analysis, and Meta-Regression. PMID: 36769504.
Weight Loss in PCOS Meta-Analysis Group. (2024). Effect of Weight Loss Interventions on the Symptomatic Burden and Biomarkers of Polycystic Ovary Syndrome: A Systematic Review of Randomized Controlled Trials. Annals of Internal Medicine, 177(12). PMID: 39496172.
Legro, R. S., et al. (2014). Letrozole versus Clomiphene for Infertility in the Polycystic Ovary Syndrome. New England Journal of Medicine, 371(2), 119-129. PMID: 25006718.
Androgen Excess Review Group. (2023). Androgen excess: a hallmark of polycystic ovary syndrome. Frontiers in Endocrinology, 14, 1273542. PMID: 38152131.
AMH-PCOS Meta-Analysis Group. (2024). Anti-mullerian hormone as a diagnostic biomarker for polycystic ovary syndrome and polycystic ovarian morphology: a systematic review and meta-analysis. Fertility and Sterility. PMID: 38944177.