Why Your Probiotic Isn’t Working (And Which One Might)
If you’ve been on a probiotic for months and you still feel bloated, gassy, or vaguely worse than before you started, you are not imagining it and you are not doing it wrong. The shelf is loud, the marketing is louder, and the part of the science that would actually help you pick the right bottle is buried in a strain code most labels do not bother to print. I read the literature on this so I could give you a real answer. Here is what I want you to know up front: probiotic efficacy is strain-specific and disease-specific, which means a bottle that worked for your friend with IBS-C may not work for you with IBS-D, and a “high-CFU multi-strain” formulation may have nothing in it that has actually been studied for what you are dealing with. CFU (colony-forming units, the count of live bacteria in one capsule) is the number on the front of every box. It is also the wrong number to make a decision with. In this piece I will walk you through what the evidence supports for IBS, for diarrhea after antibiotics, for perimenopause, and for vaginal health, plus the label-reading skill that makes all of it useful. By the end you will know what to look for, what to skip, and what to ask before you spend another fifty dollars on a bottle that does not have a strain code on it.
What does strain specificity actually mean and why does it change the question?
Strain specificity means the clinical effect of a probiotic depends on the exact strain identifier, not just the genus and species printed on the front of the bottle. If you’ve ever stood in the supplement aisle squinting at “Bifidobacterium longum” on three different products and assumed they were the same thing, that is the trap.
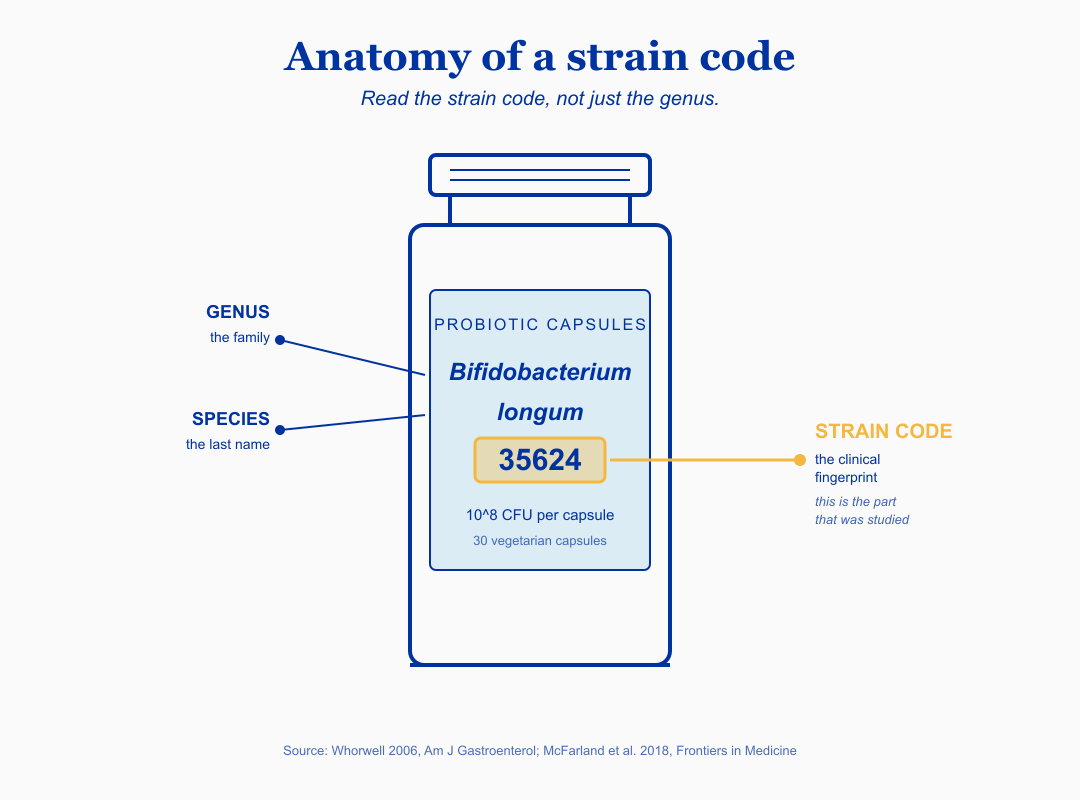
Here is the rule the literature actually supports. The genus is the family. The species is the last name. The strain identifier is the number-and-letter code after the species (for example, the “35624” in B. longum 35624) and it is the part that has been studied. A strain code is not marketing flair. It is a clinical fingerprint, because two strains of the same species can produce different short-chain fatty acid (SCFA, the small fatty acids like butyrate that your colon cells use for fuel and barrier repair) profiles, attach to different gut-lining receptors, and produce different downstream effects. A 2018 systematic review by McFarland and colleagues scoped 228 trials and concluded that strain and disease specificity are real, and that pooling probiotics together in meta-analyses obscures which strains actually do anything.
The micro-summary so far: same species, different strain code, often a very different clinical effect. The strain code is the part the evidence is about.
The shift this asks you to make is concrete. Instead of asking “is this a good probiotic,” ask “is this strain at this dose what has been studied for the exact thing I am dealing with.” That is the question the rest of this article answers, condition by condition. What this means for the woman in front of me, on her third bottle, is that the failed bottles probably were not failures of probiotics in general. They were mismatches between her actual symptom pattern and a strain that had never been studied for it.
Which probiotic strain has the strongest evidence for IBS symptoms?
If you are dealing with IBS abdominal pain, bloating, and bowel changes, the single strain with the strongest evidence is Bifidobacterium longum 35624, formerly named B. infantis 35624, taken at roughly 10^8 CFU per day for at least four weeks. This is one of the most-replicated strain-specific findings in the gut literature.
Here is the felt experience first. IBS does not just hurt in the abdomen. It eats your social calendar, makes you scan restaurant menus before you accept invitations, and quietly teaches you to plan your day around access to a bathroom. None of that shows up on lab work. That is part of why this diagnosis feels so isolating: your bloodwork is normal, your colonoscopy is clean, and your gastroenterologist may have offered you a low-FODMAP diet sheet and an antispasmodic.
The 2006 Whorwell trial in the American Journal of Gastroenterology randomized 362 women with IBS to B. infantis 35624 at three doses or placebo for four weeks. The 10^8 CFU dose was significantly superior to placebo for abdominal pain, bloating, bowel dysfunction, incomplete evacuation, straining, and gas. A 2023 network meta-analysis by Goodoory and colleagues in Gastroenterology re-confirmed this as one of the strongest single-strain signals in the IBS literature, and a 2025 strain-specific systematic review in the Journal of Clinical Medicine put B. longum 35624 in the top tier for IBS abdominal pain. To borrow the core line: B. longum 35624 at 10^8 CFU daily for 4 weeks has the strongest single-strain IBS evidence (Whorwell 2006).
The alternative with comparable evidence is Lactobacillus plantarum 299v, also called DSM 9843, at 1 to 2 capsules per day of the studied formulation for 4 weeks. Niedzielin 2001 and Ducrotte 2012 both showed reduction in abdominal pain over 4 weeks. Past four weeks the picture gets less clear, which is one of the reasons I do not present probiotics as forever supplements.
The micro-summary: for IBS pain and bloating, the two strains with the strongest evidence are B. longum 35624 (around 10^8 CFU per day, 4 weeks) and L. plantarum 299v (1 to 2 capsules per day, 4 weeks). Everything else marketed for IBS sits on weaker ground.
Patients I’ve worked with, in cases I’ve reviewed, often arrive with a multi-strain bottle that has been on the shelf for two years. The bottle contains six Lactobacillus species and no strain identifiers, and the dose is “30 billion CFU.” None of those six species have been studied as a blend for IBS at that exact ratio. What this means for the woman in front of me is that her experience of “I tried a probiotic for my IBS and it did nothing” is not evidence that probiotics fail in IBS. It is evidence that the bottle she took is not the bottle the literature is about.
Which probiotic actually prevents diarrhea when I’m on antibiotics?
For antibiotic-associated diarrhea (AAD), the two strains with the strongest evidence are Saccharomyces boulardii CNCM I-745 and Lactobacillus rhamnosus GG, each taken alongside the antibiotic course. This is also one of the few indications where major guideline bodies and the supplement industry actually agree.
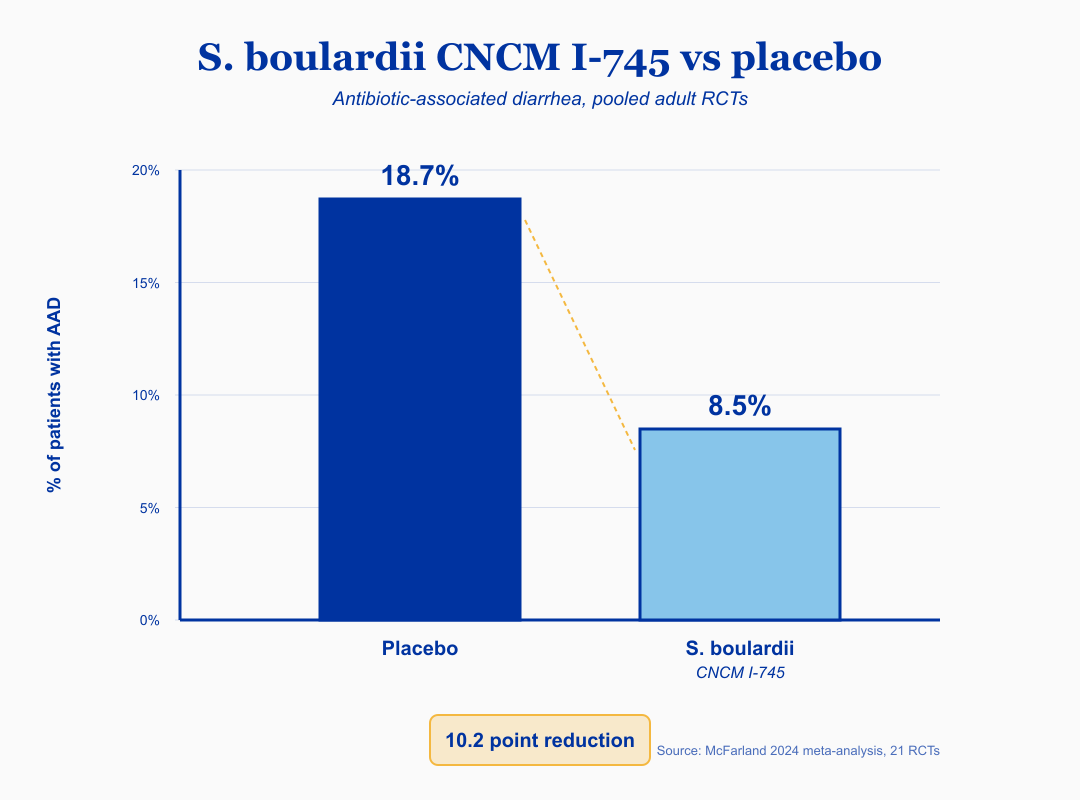
Antibiotics save lives. They also blow a hole in your gut microbial ecosystem, and roughly one in five adults who take a course of antibiotics develops diarrhea as a result. The 2024 meta-analysis pooling 21 randomized trials showed S. boulardii CNCM I-745 cuts AAD incidence from 18.7% to 8.5%, which is the line from the core artifact worth memorizing: S. boulardii CNCM I-745 cuts antibiotic-associated diarrhea from 18.7% to 8.5% in pooled adult RCTs (McFarland 2024).
The 2020 American Gastroenterological Association guideline goes a step further and explicitly recommends specific strains for C. difficile prevention in adults and children on antibiotics. The strains the AGA names map directly onto S. boulardii and certain L. rhamnosus GG-containing formulations. The strength of evidence here is the highest in this entire article. Multiple aligned systematic reviews and a major guideline body line up on the same recommendation.
The micro-summary: if you are on antibiotics and worried about diarrhea or C. difficile, the two strains the evidence and the AGA support are S. boulardii CNCM I-745 and L. rhamnosus GG. This is the indication where probiotics are most clearly evidence-based.
One practical caveat. Take the probiotic at least two to three hours apart from the antibiotic dose, because the antibiotic will kill the probiotic if they meet in your stomach. And note that S. boulardii is a yeast, not a bacterium, which is why systemic antifungal medications are a contraindication. What this means for the woman in front of me is that the pharmacy-counter advice to “take a probiotic with your antibiotic” is closer to right than wrong, as long as the strain is one of these two and the spacing is respected.
“Most women come in with a multi-strain probiotic they have been taking for years for bloating, and not one of the strains in that bottle has been studied for IBS at the dose they are taking. What is worse is that the probiotic they are taking is actually worsening the symptoms. I have seen this to cause a lot of mental distress in my patients.
Does the strain identifier on the label even mean anything if the bottle does not contain it?
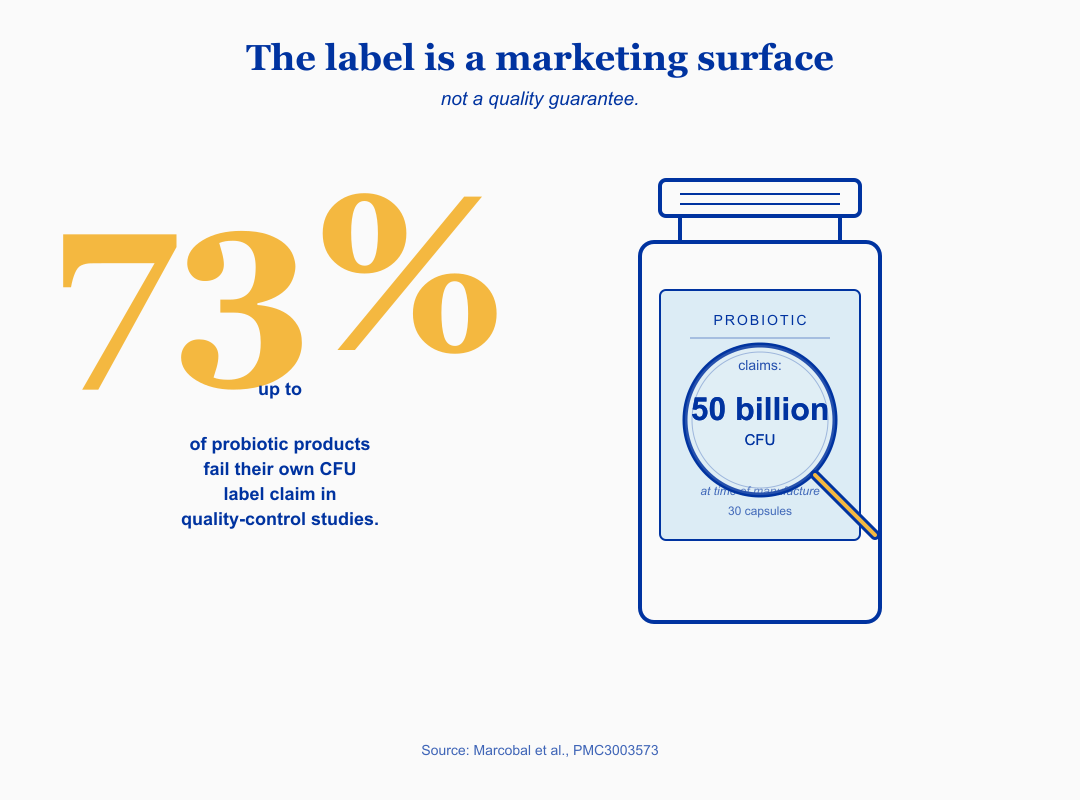
This is the part of the probiotic conversation that the supplement industry would rather you skip. Multiple quality-control studies have shown that up to 73% of probiotic products fail to meet their own CFU label claim by the end of shelf life, and roughly 32% of products with specific organism claims have misspelled the species name on the label.
The strain you read about in a clinical trial is one specimen of one organism, deposited in a culture collection, with a paper trail. The strain in a generic supermarket multi-strain bottle is, in some cases, not the same organism, and in some cases, not viable. A 2008 to 2010 assessment by Marcobal and colleagues, found that only 4 of 15 products with specific viability claims met or exceeded their label claim, and one product had zero detectable live organisms despite claiming 14 million CFU per capsule. The line from the core artifact, verbatim: Up to 73% of probiotic products fail their own CFU label claim in quality-control studies (Marcobal et al., PMC3003573).
The micro-summary: the label is a marketing surface, not a quality guarantee. The strain code is the only signal that someone has even tried to tell you what is inside the capsule.
What to look for, practically. Look for the strain identifier (the letters and numbers after the species), not just the genus and species. Look for third-party testing seals such as USP, NSF, or ConsumerLab. Look for “guaranteed CFU at end of shelf life” rather than “CFU at time of manufacture.” Avoid “proprietary blends” that hide strain identities. Patients I’ve worked with often discover, the first time someone reads the label closely with them, that the bottle they have been buying for two years lists six species and zero strain codes. What this means for the woman in front of me is that the literature does not yet apply to her, because what she has been taking is not what the literature studied.
Is “always take a probiotic after antibiotics” actually true?
This is the part of the conversation where the wellness world and the literature diverge most sharply. The intuitive logic (“antibiotics killed bacteria, so add bacteria back”) is appealing. The evidence is more complicated. A 2018 study by Suez and colleagues in the journal Cell showed that a multi-strain probiotic taken after a course of antibiotics actually delayed indigenous gut microbiome reconstitution for up to six months in humans, while autologous fecal microbiota transfer restored it within days.
That is one rigorous study, not a replicated body of work, and I do not want to overstate it. But the implication matters. If you are taking a generic multi-strain probiotic after antibiotics on the assumption that it is “restoring” your microbiome, the picture may be more nuanced than that. The strains in the bottle may be occupying niches that your own indigenous bacteria would otherwise refill on their own.
This is the place where strain and indication matter most. The AGA 2020 guideline still recommends specific strains during antibiotic therapy for C. difficile prevention. That is a different question from “should I take a generic multi-strain after antibiotics to rebuild my gut.” The first has strong evidence. The second has emerging counter-evidence from one important paper.
The micro-summary: take a studied strain (S. boulardii CNCM I-745 or L. rhamnosus GG) during antibiotics for diarrhea and C. difficile prevention. Be cautious about a generic multi-strain “rebuild” approach after antibiotics. The picture is more complicated than the supplement aisle tells you.
What this means for the woman in front of me is that the question is not “do I take a probiotic with my antibiotic” but “which strain, at which time, for which outcome.” The first question has a yes-or-no answer in the supplement aisle. The second question is the one the evidence actually answers, but may also need further guidance from her physician.
Which probiotics have evidence for perimenopause and bacterial vaginosis?
For perimenopausal vasomotor symptoms (hot flashes and night sweats) and for bacterial vaginosis (BV, an overgrowth of anaerobic bacteria in the vaginal microbiome that causes odor, discharge, and recurrent infection), the strain story is genuinely interesting and genuinely unsettled.
For perimenopause specifically, a 2025 systematic review and meta-analysis in Heliyon pooled seven randomized trials of multi-strain Lactobacillus + Bifidobacterium formulations in perimenopausal and menopausal women and found a large effect on vasomotor symptoms (standardized mean difference around -0.96), a moderate effect on psychological symptoms, and improvement in vaginal dryness. That is a strong signal in a population that has been told for decades to wait it out. The caveat is that the strain composition varied across the seven trials, which means the meta-analysis tells you “probiotics in this category help” but does not yet tell you “this specific strain at this specific dose is the one.”
The body went through a hormonal recalibration without telling you. The night sweats wake you at 3am, the brain fog makes you second-guess yourself in meetings, and the vaginal dryness changes how you experience intimacy. None of that is in your head. What the 2025 meta-analysis adds is that for some women, a multi-strain Lactobacillus + Bifidobacterium formulation may be part of the toolkit alongside whatever else you and your doctor decide on.
For recurrent bacterial vaginosis, oral Lactobacillus rhamnosus GR-1 + Lactobacillus reuteri RC-14 has been studied as an adjunct to standard antibiotic therapy (metronidazole or tinidazole). The 2006 Anukam trial and the 2009 Martinez trial both showed cure rate improvements with the combination over antibiotic alone, in the range of 87 to 88% versus 40 to 50%. A 2021 Chinese cohort study showed no added benefit, which is an honest heterogeneity flag. The signal is real, the population-specific variation is real, and a single global recommendation does not yet exist.
The micro-summary: for perimenopause vasomotor symptoms, a 2025 meta-analysis supports multi-strain Lactobacillus + Bifidobacterium formulations with a large effect size, with strain composition still heterogeneous. For BV, the GR-1 + RC-14 oral adjunct has supportive RCTs and one null cohort study.
What this means for the woman in front of me is that if you are in perimenopause and your night sweats are stealing your sleep, the literature does not yet hand you one perfect strain identifier, but it does hand you a category that is worth a conversation with your provider. And if you have recurrent BV and you are tired of cycling through metronidazole every three months, the oral GR-1 + RC-14 adjunct is a real thing the literature points to.
When should I not take a probiotic?
The answer most influencer content does not give you. Probiotics are generally safe in healthy adults at standard doses, but there are populations where the risk-benefit shifts hard.
Severely immunocompromised states are an absolute caution. That includes post-transplant patients, patients with advanced HIV and low CD4 counts, neutropenic patients, and patients with severe inflammatory bowel disease with active mucosal breach. The Lactobacillus bacteremia rate in ICU patients receiving L. rhamnosus GG has been reported around 1.1%, compared with 0.009% in controls. Case reports of fungemia with S. boulardii in critically ill patients with central venous catheters also exist. This is not a hypothetical risk in this population. If you or someone you care for is in any of these categories, do not start a probiotic without explicit guidance from the treating team.
Pregnancy is a softer caveat. The accumulated evidence base across roughly 1,500 documented pregnancy exposures to Lactobacillus and Bifidobacterium showed no clear fetal harm signal in earlier reviews. A 2025 meta-analysis in the journal Medicine raised a possible elevated preeclampsia (a hypertensive complication of pregnancy with proteinuria) signal in probiotic-supplemented pregnancies. That finding is recent and not yet adjudicated by guideline bodies. The practical rule is to talk to your obstetric provider before starting any new supplement during pregnancy, including a probiotic, even if a previous provider was comfortable with it.
SIBO (small intestinal bacterial overgrowth, where bacteria that normally live in the colon proliferate higher up in the small intestine) is a relative caution. Some probiotic strains and prebiotic-containing formulations can worsen SIBO symptoms in some patients. A 2018 case series by Rao and colleagues described probiotic-associated D-lactic acidosis and brain fog in a subset of SIBO patients. The methodology has been criticized but the signal is worth taking seriously if you are SIBO-positive and feel worse on probiotics.
The micro-summary: probiotics are generally safe in healthy adults but require a real conversation with your provider if you are immunocompromised, pregnant, or SIBO-positive. Third-party testing matters because the bottle may not be what the label claims.
What this means for the woman in front of me, on her fourth probiotic and feeling worse, is that the next question is not “which strain do I try next” but “is there something else going on that the probiotic is exacerbating.” That is a conversation worth having with the clinician who knows your history, not with the supplement aisle.
What I’d do this week
Here is the save card from this piece. Screenshot it, bring it to your pharmacist or your doctor, and use it as the starting point for a real conversation. None of this is medical advice for your specific situation; it is the synthesis of what the literature supports as of May 2026.
Which probiotic for which problem
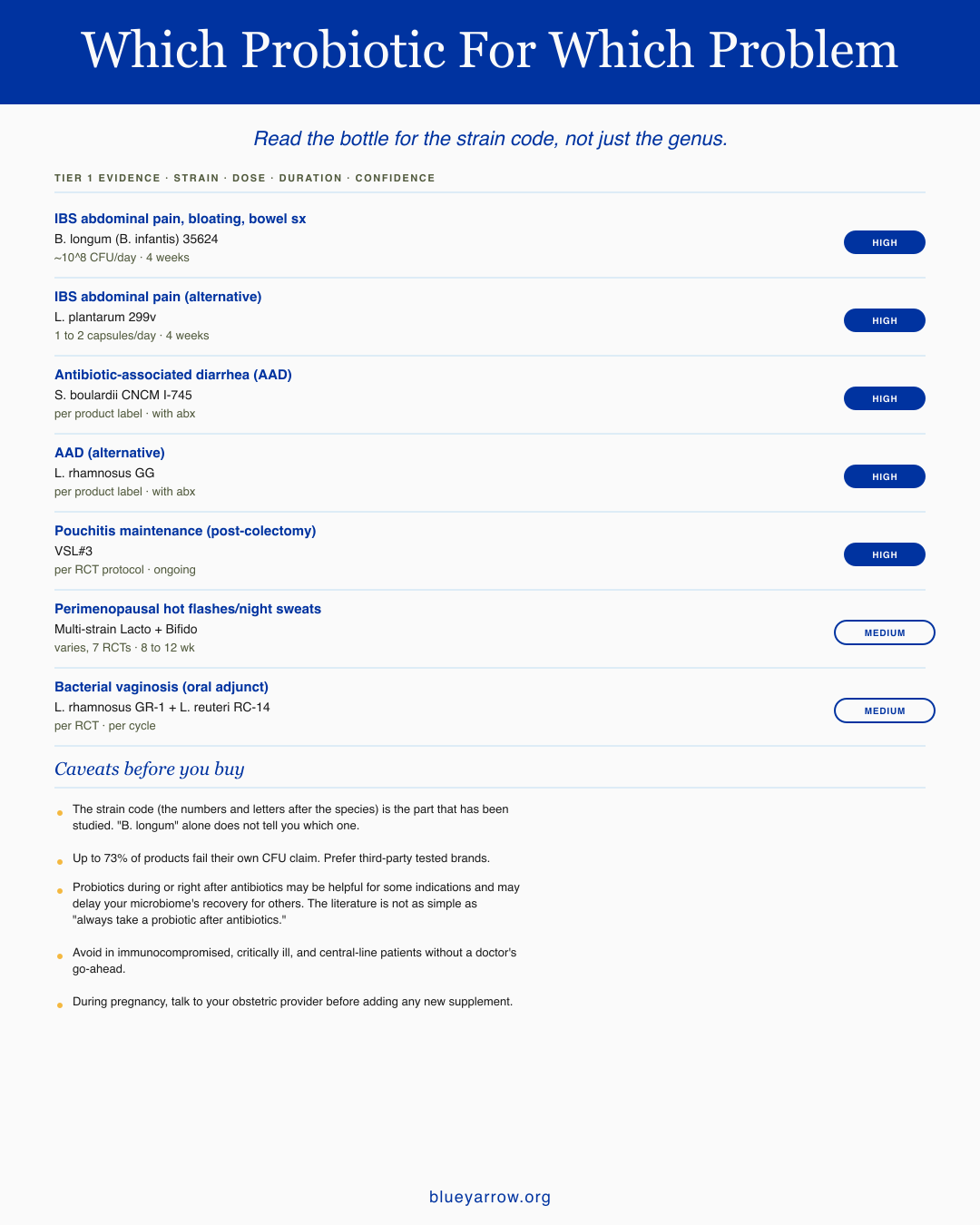
The strains with Tier 1 evidence. Read the bottle for the strain code, not just the genus.
For IBS (abdominal pain, bloating, bowel changes)
Primary: B. longum subspecies infantis 35624 at roughly 10^8 CFU per day for 4 weeks.
Alternative: L. plantarum 299v at 1 to 2 capsules per day for 4 weeks.
Both have solid trial data behind them.
For antibiotic-associated diarrhea (AAD)
Primary: S. boulardii CNCM I-745 per the product label, taken alongside your antibiotic course.
Alternative: L. rhamnosus GG per the product label, same approach.
Strong evidence for both as adjuncts.
For pouchitis maintenance (post-colectomy)
Primary: VSL#3 per the RCT dosing protocol, ongoing.
This is the one strain combination with consistent maintenance data in this specific population.
For perimenopausal hot flashes and night sweats
Primary: Multi-strain Lacto + Bifido formulations, dosing varies by product, 8 to 12 weeks.
The evidence is solid but the seven studies use different formulations, so confidence is moderate rather than high.
For bacterial vaginosis (oral adjunct to standard treatment)
Primary: L. rhamnosus GR-1 + L. reuteri RC-14 per the RCT protocol, used per cycle.
Moderate confidence — this is an adjunct to standard care, not a replacement.
Caveats before you buy:
The strain code matters. The numbers and letters after the species name (the "35624" or "CNCM I-745" part) are what was actually studied. "B. longum" by itself tells you nothing. There are thousands of strains within a species, and almost none of them have the trial data.
Up to 73 percent of probiotic products fail their own CFU claim when third-party tested. Prefer brands that have been verified by USP, NSF, or ConsumerLab.
Probiotics during or right after antibiotics is more nuanced than the wellness internet makes it sound. For some indications they help. For others, they may actually delay your microbiome's recovery. The literature is not "always take a probiotic after antibiotics."
Avoid probiotics if you are immunocompromised, critically ill, or have a central line, without a doctor's go-ahead. During pregnancy, talk to your obstetric provider before adding any new supplement.
The three actions for this week. First, pull whatever probiotic bottle is on your kitchen counter and find the strain identifier. If there is no identifier (only genus and species), set the bottle aside. Second, write the exact symptom you bought it for. Third, compare to the table above. If the strain matches the symptom, you may be in the right place. If not, the next conversation is with your provider.
A note on what I do and do not recommend
I built Blue Yarrow because I want to share my naturopathic doctor training and knowledge so that people who aren’t getting answers from conventional doctors can find the answers with me. That is a teaching mission, not a prescribing one. Nothing in this piece is a personalized recommendation. What I share with people who ask me about probiotics is exactly what is on this page: the strain identifier matters more than the CFU number, the indication matters more than the brand, and the conversation with your provider is the part that turns the literature into a decision for your body.
Frequently asked questions
Is more CFU always better? Not according to the evidence. A 2022 meta-analysis in IBS found no overall dose-response relationship between CFU count and symptom relief across products. Strain choice and matching to your specific symptom outweighs total CFU number. The bottle with the highest CFU is often the easiest one to market, not the best one to take.
Are probiotics safe to take with antibiotics? For specific strains, yes, and the AGA 2020 guideline supports this for C. difficile prevention. The two strains with the strongest evidence are S. boulardii CNCM I-745 and L. rhamnosus GG. Separate the probiotic dose from the antibiotic dose by two to three hours so the antibiotic does not kill the probiotic in your stomach.
Can probiotics make IBS worse? For some people, yes. If you are SIBO-positive, prebiotic-containing formulations and certain D-lactate-producing strains may aggravate symptoms. If you started a probiotic and felt worse, that experience is real and worth bringing to your provider rather than pushing through.
Are probiotics safe during pregnancy? Most accumulated data on Lactobacillus and Bifidobacterium in pregnancy is reassuring, but a 2025 meta-analysis raised a possible preeclampsia signal that is not yet adjudicated. Talk to your obstetric provider before starting any new supplement during pregnancy, including a probiotic.
Can I get probiotics from food instead of pills? Yes for general digestive support, and the evidence supports fermented foods (yogurt, kefir, sauerkraut, kimchi) as part of a varied diet. For specific indications like IBS or AAD prevention, fermented foods do not deliver the specific strains at the specific doses studied in the trials, so food and supplements are different tools for different questions.
What does the strain code on the label mean? The strain code is the letters and numbers after the species name (for example, the “35624” in B. longum 35624 or the “CNCM I-745” in S. boulardii CNCM I-745). It identifies the exact organism deposited in a culture collection and studied in clinical trials. Without it, you cannot tell whether the bottle contains the strain the literature is about.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
What did this piece clarify for you, and which strain decision are you still stuck on?
References
McFarland, L. V., Evans, C. T., and Goldstein, E. J. C. (2018). Strain-specificity and disease-specificity of probiotic efficacy: A systematic review and meta-analysis. Frontiers in Medicine, 5, 124. https://doi.org/10.3389/fmed.2018.00124
Whorwell, P. J., Altringer, L., Morel, J., Bond, Y., Charbonneau, D., O’Mahony, L., Kiely, B., Shanahan, F., and Quigley, E. M. M. (2006). Efficacy of an encapsulated probiotic Bifidobacterium infantis 35624 in women with irritable bowel syndrome. American Journal of Gastroenterology, 101(7), 1581-1590.
Niedzielin, K., Kordecki, H., and Birkenfeld, B. (2001). A controlled, double-blind, randomized study on the efficacy of Lactobacillus plantarum 299V in patients with irritable bowel syndrome. European Journal of Gastroenterology and Hepatology, 13(10), 1143-1147.
Ducrotte, P., Sawant, P., and Jayanthi, V. (2012). Clinical trial: Lactobacillus plantarum 299v (DSM 9843) improves symptoms of irritable bowel syndrome. World Journal of Gastroenterology, 18(30), 4012-4018.
Goodoory, V. C., Khasawneh, M., Black, C. J., Quigley, E. M. M., Moayyedi, P., and Ford, A. C. (2023). Efficacy of probiotics in irritable bowel syndrome: A network meta-analysis. Gastroenterology. https://doi.org/10.1053/j.gastro.2023.04.032
Madempudi, R. S., Neelamraju, J., Ahire, J. J., Gupta, S. K., and Shukla, V. K. (2019). Bacillus coagulans Unique IS2 in IBS: A double-blind, randomized, placebo-controlled study. Scientific Reports, 9, 12210. https://doi.org/10.1038/s41598-019-48554-x
Su, G. L., Ko, C. W., Bercik, P., Falck-Ytter, Y., Sultan, S., Weizman, A. V., and Morgan, R. L. (2020). AGA clinical practice guidelines on the role of probiotics in the management of gastrointestinal disorders. Gastroenterology, 159(2), 697-705. https://doi.org/10.1053/j.gastro.2020.05.059
Lacy, B. E., Pimentel, M., Brenner, D. M., Chey, W. D., Keefer, L. A., Long, M. D., and Moshiree, B. (2021). ACG clinical guideline: Management of irritable bowel syndrome. American Journal of Gastroenterology, 116(1), 17-44.
World Gastroenterology Organisation. (2023). WGO practice guideline: Probiotics and prebiotics.
Suez, J., Zmora, N., Zilberman-Schapira, G., Mor, U., Dori-Bachash, M., Bashiardes, S., et al. (2018). Post-antibiotic gut mucosal microbiome reconstitution is impaired by probiotics and improved by autologous FMT. Cell, 174(6), 1406-1423.e16. https://doi.org/10.1016/j.cell.2018.08.041
Schnadower, D., Tarr, P. I., Casper, T. C., et al. (2018). Lactobacillus rhamnosus GG versus placebo for acute gastroenteritis in children. New England Journal of Medicine, 379, 2002-2014. https://doi.org/10.1056/NEJMoa1802598
Anukam, K., Osazuwa, E., Ahonkhai, I., Ngwu, M., Osemene, G., Bruce, A. W., and Reid, G. (2006). Augmentation of antimicrobial metronidazole therapy of bacterial vaginosis with oral probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14. Microbes and Infection, 8(6), 1450-1454.
Rao, S. S. C., Rehman, A., Yu, S., and Andino, N. M. (2018). Brain fogginess, gas and bloating: A link between SIBO, probiotics and metabolic acidosis. Clinical and Translational Gastroenterology, 9(6), 162. https://doi.org/10.1038/s41424-018-0030-7
Marcobal, A., Underwood, M. A., and Mills, D. A. (2008-2010 reference set). Assessment of commercial probiotic bacterial contents and label accuracy. PMC3003573.
Hill, C., Guarner, F., Reid, G., Gibson, G. R., Merenstein, D. J., Pot, B., et al. (2014). The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nature Reviews Gastroenterology and Hepatology, 11(8), 506-514.
Investigating the effects of probiotics during the menopause transition: A systematic review and meta-analysis. (2025). Heliyon. PMID: 40639456.
Mardini, H. E., and Grigorian, A. Y. (2014). Probiotic mix VSL#3 is effective adjunctive therapy for mild to moderately active ulcerative colitis: A meta-analysis. Inflammatory Bowel Diseases, 20(9), 1562-1567.
Markowiak-Kopec, P., and Slizewska, K. (2020). The effect of probiotics on the production of short-chain fatty acids by human intestinal microbiome. Nutrients, 12(4), 1107. https://doi.org/10.3390/nu12041107