Why a Normal Mold Panel Doesn’t Mean You’re Fine
Your doctor ran a mold allergy test. It came back normal, and you got sent home knowing something the test did not. You still react to wine. Aged cheese wrecks you now in a way it never used to. Your heart races after dinner. The flushing shows up before your period and nobody could tell you why. So you went looking, and the internet handed you a clean story about mold toxins poisoning you through the air. Here is what conventional medicine misses here, and what the wellness world oversells.
A standard mold allergy panel was built to find one specific thing. It was not built to measure how much histamine your body is carrying or how well your gut clears it. So a normal result rules out an allergy. It does not rule out you. I am going to walk you through what that panel actually measures and why a damp home makes these symptoms worse. Then I will show you where the popular mycotoxin test falls apart. Then I will give you exactly what I would do this week.
What does a normal mold allergy panel actually measure?
A normal mold allergy panel measures IgE allergy, not your total histamine load. That single sentence is the whole problem. The test was designed to catch one immune pathway. Your symptoms may be running down a different one entirely.
If you have been told you are fine, I want to name what that felt like first. You walked in with a real pattern of symptoms and walked out with a normal result and no explanation. That is not nothing. That is being mismeasured, which is different from being healthy.
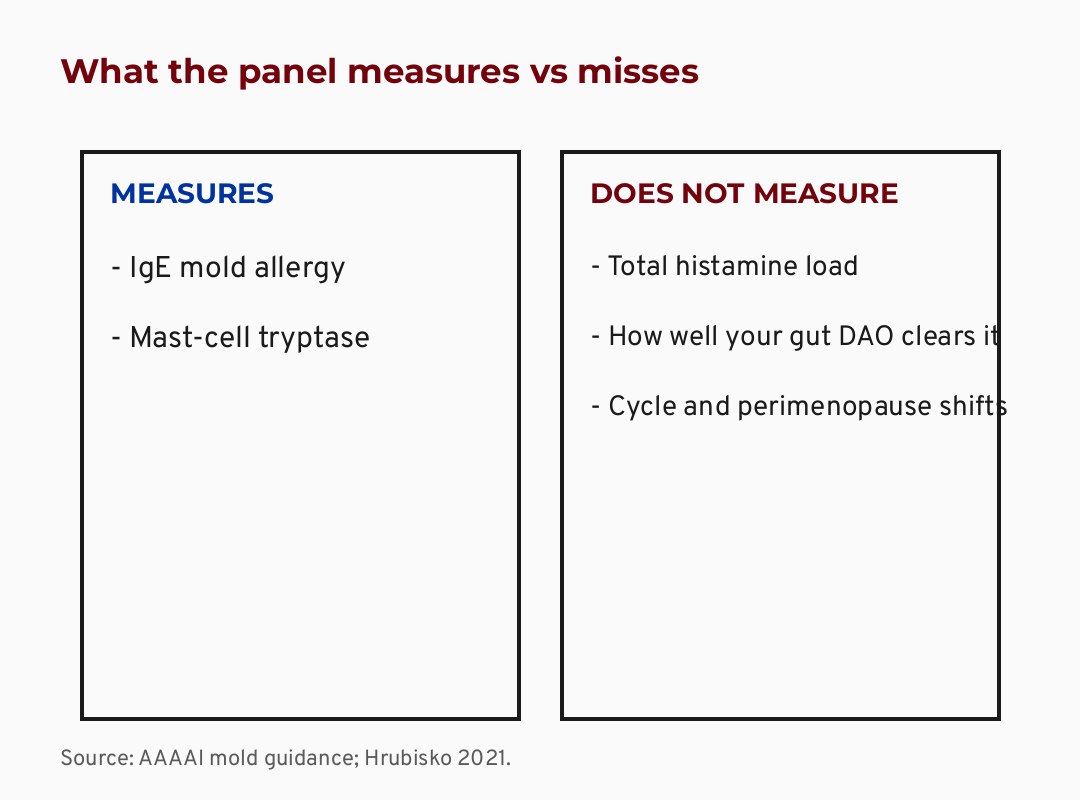
Let me explain what the panel does. An IgE panel checks whether your body has built an allergy to mold. An IgE panel is a blood or skin test. It looks for the specific antibody your immune system makes during a classic allergic reaction. Your doctor may also run tryptase. Tryptase (an enzyme released when mast cells fire heavily, used as a marker of allergic and mast-cell activity) tells them about mast-cell load. Both are real tests. Both answer a narrow question.
Here is the part most people never hear. A normal IgE mold panel measures allergy, not your total histamine load (AAAAI; Hrubisko 2021). Mast cells are the immune cells that store and release histamine. Histamine is a signaling molecule your body uses for immune response, stomach acid, and alertness. It has to be broken down after it does its job. The allergy panel does not look at how much histamine is in circulation or how fast you clear it. So the test can be perfectly normal while your histamine handling is not.
The short version: a normal allergy panel rules out IgE allergy. It does not rule out a histamine-load pattern, because those are two different questions and the panel only answers one.
Why does a damp or moldy home make this worse?
Living in a damp or moldy home raises the risk of allergic and histamine-type symptoms in susceptible people. The signal is strongest when there is a musty smell. This is the part the evidence actually supports, and it is worth holding onto.
Maybe you have stood in your own house and thought “I feel allergic to my own home.” That instinct is not irrational. The data backs the pattern, even if your allergy test did not.
Here is what the research shows. Visible household mold raises rhinitis risk 82 percent, and a musty smell raises it more (Jaakkola 2013). Rhinitis is the medical word for the runny, stuffy, sneezy nasal symptoms most people call allergies. Three separate meta-analyses point the same direction. Jaakkola 2013 pooled 31 studies and found visible mold raised rhinitis risk, with mold odor carrying the strongest signal of all. Quansah 2012 found a similar pattern for new-onset asthma.
I want to be honest about the limit here, because the honesty is the point. Most of these studies are cross-sectional, which means they captured mold and symptoms at one moment instead of following people over time. The effect sizes are modest. The link is real and consistent across countries and study designs, but it is an association, not airtight proof of cause. That matters for what you do next. It is exactly why chasing a single biomarker is the wrong move, and addressing the exposure is the right one.
The root-cause version of this question is not “which supplement neutralizes the mold.” It is “what in my environment is loading my system, and can I remove it.” A musty smell is your strongest lever. Not a test. A smell.
The short version: damp homes genuinely worsen histamine-type symptoms in susceptible people, and the musty-smell signal is the strongest. The evidence is real but observational, which is why the exposure matters more than any biomarker.
What is histamine intolerance, and why is it so hard to diagnose?
Histamine intolerance is a recognized pattern tied largely to how well the gut enzyme DAO breaks down the histamine you eat. It is genuinely hard to diagnose because the symptoms are nonspecific. That difficulty is most of the reason you were missed.
Maybe you have started reacting to foods you used to love. Maybe a doctor waved it off because your tests looked normal. That frustration is earned. The tests were probably looking in the wrong place.
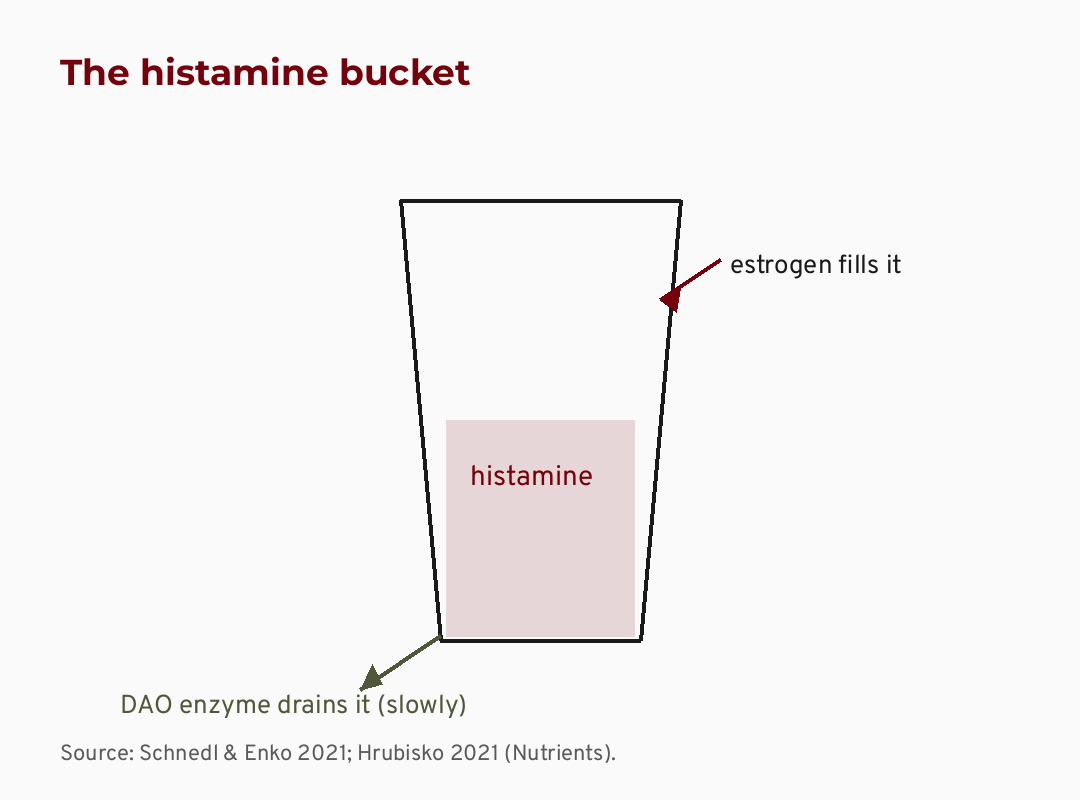
Let me explain the mechanism plainly. DAO stands for diamine oxidase. DAO (the main gut enzyme that breaks down histamine from food before it enters your bloodstream) is your first line of defense against dietary histamine. Histamine intolerance is a gut DAO-enzyme problem, confirmed across two 2021 Nutrients reviews (Schnedl, Hrubisko). When DAO activity is low, histamine from food builds up instead of clearing. Aged cheese, wine, fermented foods, and leftovers are all high in histamine. That is why they hit hardest.
This is where the naturopathic lens on this changes the whole conversation. Conventional care asks “is there an allergy, yes or no.” That is a binary. The root-cause question is different. It asks how well your body is processing and clearing histamine in the first place, which is a system, not a yes-or-no. A patient I worked with described it as a bucket. Her bucket was full, so the glass of wine that used to be fine was now the overflow. That image is more accurate than most lab reports she had been handed.
In cases I have reviewed, the pattern is consistent. Flushing, a racing heart after meals, headaches, loose stools, and reactions to exactly the foods highest in histamine. No single test confirms it cleanly, which is precisely why it slips through a ten-minute appointment.
The short version: histamine intolerance centers on the gut enzyme DAO, not on a classic allergy. It is hard to diagnose because the symptoms are vague and no single blood test nails it. That is why so many women get told they are fine.
Is it menopause or is it mold? The hormone overlap
Histamine symptoms can shift across your menstrual cycle and intensify in perimenopause. Estrogen and progesterone affect how much histamine your mast cells release and how fast your body clears it. If your symptoms track your cycle, take that seriously.
If you have caught yourself asking “is this menopause or is it mold,” I want to validate that you are asking a smart question. The honest answer is that it can genuinely be both at once, and the hormone piece is real even if it is not fully proven.
Here is the physiology, and here is where I am going to be careful with my language. Perimenopause is the years-long hormonal transition before your periods stop, when estrogen and progesterone swing unpredictably. Estrogen tends to push mast cells to release more histamine and appears to lower DAO activity. Progesterone seems to do the opposite. So when your hormones swing, your histamine handling can swing with them.
I want to be clear that this is plausible physiology, not proven causation. The mechanism is biologically coherent and described consistently in the literature, including Theoharides 2019. What we do not have is strong human-outcome data in women your age tying estrogen levels to measured histamine symptoms over time. So I will say it may explain why your symptoms worsen the week before your period or intensify in your late thirties and forties. I will not tell you it is settled science. The honesty here is not me hedging. It is me respecting your intelligence enough to tell you where the evidence stops.
What this means for the woman in front of me is simple. If your reactions get worse premenstrually or have ramped up during perimenopause, that is a real and recognized pattern. It is a reason to take your symptoms seriously, not a license for anyone to hand you a mold-toxicity diagnosis.
The short version: estrogen and progesterone genuinely influence histamine, so symptoms can swing with your cycle and intensify in perimenopause. The mechanism is plausible and worth respecting, but it is not proven causation, so treat it as a clue, not a verdict.
Is the urine mycotoxin test worth the money?
A positive urine mycotoxin test is not a diagnosis. Most healthy people test positive from food alone, so a positive result on its own proves very little.
I know this one stings, because for a lot of women that test felt like the first real answer anyone gave them. I am not here to take your answer away. I am here to make sure the answer you build on can actually hold weight.
Let me explain what a mycotoxin is and where the test goes wrong. A mycotoxin is a compound some molds produce. It also shows up in common foods like grains, coffee, and dried fruit. So it is not unique to a sick body. Because mycotoxins enter through ordinary diet, most healthy people test positive in their urine. There is no validated healthy baseline to compare your result against. Without a baseline, a positive number cannot separate sick from well.
There is a bigger claim underneath this test, and it does not hold. The story that inhaled mold toxins flood your body with histamine and poison you systemically is not supported by the evidence. In August 2025, the American College of Medical Toxicology weighed in. Indoor inhaled mycotoxin doses are generally far below the threshold needed to cause systemic toxicity. The real, well-documented harm from a damp home is allergic and respiratory, not toxic poisoning.
This is the trust-building part, so I want to be direct. The wellness world sells this test hardest precisely because a positive result feels like vindication after years of being dismissed. I understand the pull. But a test that flags positive in healthy people, with no validated baseline, cannot be the foundation of your plan. Skipping it as proof is not me siding with the doctors who failed you. It is me refusing to sell you a different oversimplification.
The short version: the urine mycotoxin test reads positive in most healthy people from diet alone, with no validated baseline. A positive result is not a diagnosis. The inhaled-mold-poisoning story is not supported by current toxicology.
A quick word about MCAS and binders
If you have been reading about mold and histamine, you have almost certainly run into two more things. MCAS and “binders.” Both deserve a careful, honest word before you act on either.
MCAS stands for mast cell activation syndrome. MCAS (a condition where mast cells release their mediators inappropriately and repeatedly) is real, but how common it is remains genuinely contested. One group estimates it may affect up to 17 percent of the population. The leading allergy body uses much stricter criteria and warns that the broad definition labels many people who likely have something else. I am not going to diagnose you with MCAS from a blog, and I would be cautious about anyone who diagnoses you with it quickly. That contradiction in the literature is real, and you deserve to know it exists rather than have it smoothed over.
Binders are the other piece. Binders are products like cholestyramine, charcoal, and clay, marketed in mold protocols to “pull toxins out.” Here is the honest take. They are not benign. They bind many oral medications and fat-soluble vitamins right along with whatever else. That is a real interaction risk. And they have no validated efficacy for mold detox. I would not start one casually, and I would never start one without a clinician who knows your full medication list.
The short version: MCAS is real but its prevalence is genuinely disputed, so be wary of a fast diagnosis. Binders carry real interaction risk and no proven mold benefit, so they are not a casual self-experiment.
What I’d do this week
Before any protocol, I want to give you the one-page version you can actually use. This is the artifact I wish someone had handed you at that first normal-result appointment. Save it for your next doctor visit.
Your mold panel was normal. Here’s how to read what’s actually happening.
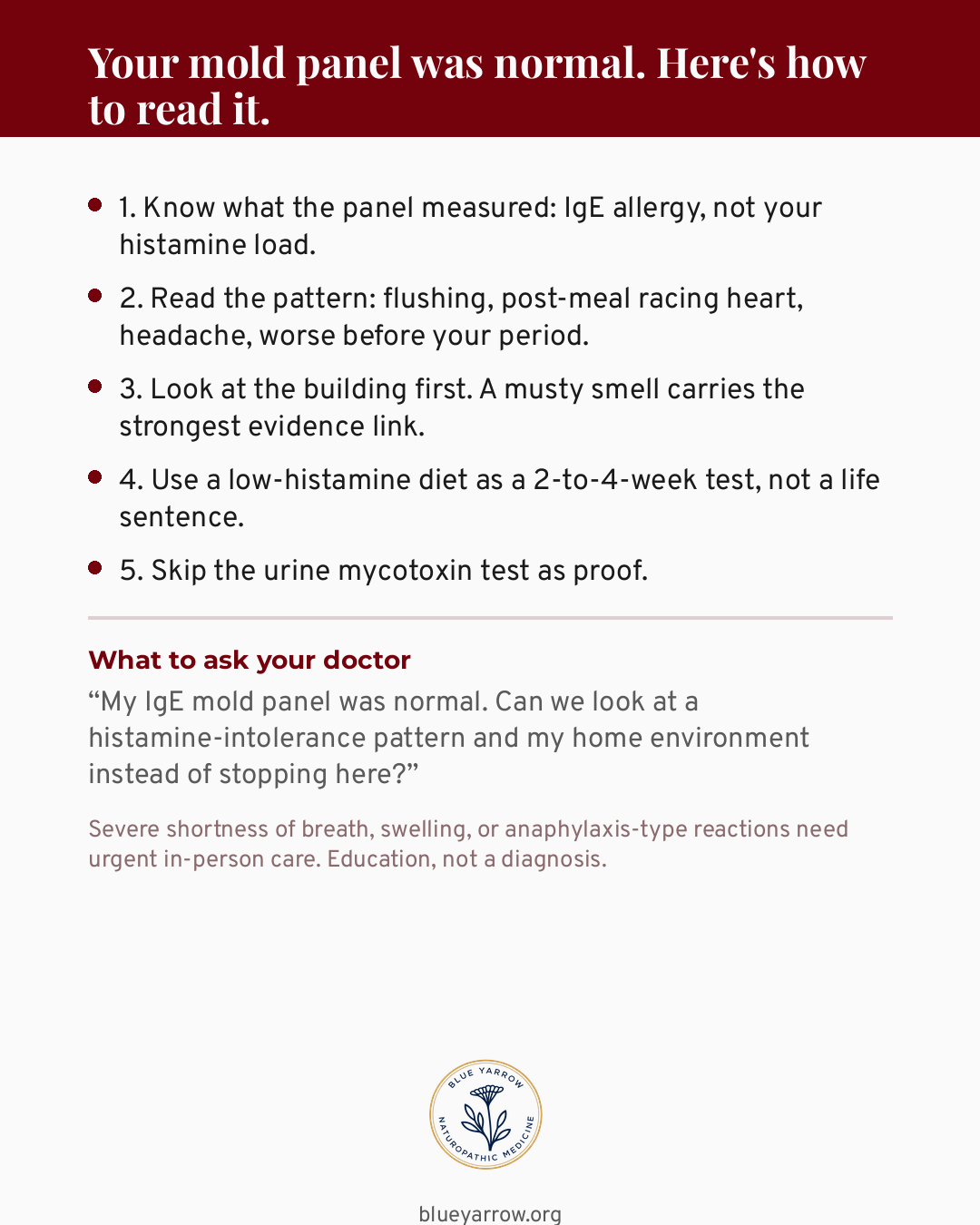
One caution: Severe shortness of breath, swelling, or anaphylaxis-type reactions need urgent in-person care, not a checklist. This is education, not a diagnosis.
A note on that low-histamine diet, because it is the step most easily misused. It works as a short diagnostic trial. If your symptoms ease over two to four weeks, that supports the histamine pattern. It is not a permanent way to eat. Long-term restriction risks real nutritional gaps and can slide into disordered eating. The goal is information, then reintroduction. Not a life lived around a food list.
The short version: read the pattern and fix the building first. Use the diet as a short test, ask your doctor the one question that reopens the conversation, and skip the urine test as proof.
The bottom line
You were not imagining it, and you were not fine. You were mismeasured. A normal allergy panel answered a narrow question and got read as a verdict on your whole body. The dampness link is real, and the histamine pattern is real. The hormonal swing that makes it worse before your period is a recognized clue worth taking seriously.
The third position here is the one nobody is selling you. You do not have to choose between a doctor who dismisses you and a test that overpromises. You can validate the symptom, read the pattern, and fix the exposure. You can run a short diet trial and refuse the test that cannot tell you anything. That is the calm, honest middle, and it is where the real answers live.
What did your doctor say when you asked about your mold result? I would genuinely like to know. The gap between what you felt and what the test reported is exactly the gap I built Blue Yarrow to close.
Frequently asked questions
Can you have a mold-related histamine problem with a normal allergy test? Yes. A standard IgE mold panel checks for classic allergy, not how well your gut clears histamine. A normal result rules out an allergy. It does not rule out a histamine-load pattern, which runs through a different mechanism the allergy panel was never built to measure.
Does a damp home really cause histamine symptoms? Damp and moldy homes raise the risk of allergic and histamine-type symptoms in susceptible people. The signal is strongest when there is a musty smell (Jaakkola 2013). The evidence is consistent but largely observational, so addressing the exposure matters more than chasing a single test result.
Is the urine mycotoxin test accurate for diagnosing mold illness? No. Most healthy people test positive for urinary mycotoxins from food alone, and there is no validated healthy baseline to compare against. A positive result feels like an answer. On its own it cannot separate a sick person from a well one, so it is not a diagnosis.
Why did my histamine symptoms start in my late thirties or forties? Estrogen and progesterone influence how much histamine your mast cells release and how fast you clear it. As hormones swing through perimenopause, histamine symptoms can intensify. This is plausible physiology rather than proven causation, but it is a recognized pattern, especially when symptoms worsen before your period.
Will a low-histamine diet cure histamine intolerance? No. A low-histamine diet works best as a 2-to-4-week diagnostic trial. If your symptoms ease, that supports the pattern. Long-term restriction is not a cure and carries real nutritional risk, so the goal is short-term information followed by careful reintroduction, not permanent restriction.
Should I take binders to detox from mold? Be cautious. Binders like cholestyramine, charcoal, and clay bind many medications and fat-soluble vitamins. That is a genuine interaction risk, and they have no validated efficacy for mold detox. They are not benign, so they are not a safe casual self-experiment without a clinician who knows your full medication list.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Citations
1. Jaakkola, M. S., Quansah, R., Hugg, T. T., Heikkinen, S. A. M., & Jaakkola, J. J. K. (2013). Association of indoor dampness and molds with rhinitis risk: A systematic review and meta-analysis. Journal of Allergy and Clinical Immunology, 132(5), 1099-1110.e18. https://doi.org/10.1016/j.jaci.2013.07.028
2. Quansah, R., Jaakkola, M. S., Hugg, T. T., Heikkinen, S. A. M., & Jaakkola, J. J. K. (2012). Residential dampness and molds and the risk of developing asthma: A systematic review and meta-analysis. PLoS One, 7(11), e47526. https://doi.org/10.1371/journal.pone.0047526
3. Hrubisko, M., Danis, R., Huorka, M., & Wawruch, M. (2021). Histamine intolerance: The more we know the less we know. A review. Nutrients, 13(7), 2228. https://doi.org/10.3390/nu13072228
4. Schnedl, W. J., & Enko, D. (2021). Histamine intolerance originates in the gut. Nutrients, 13(4), 1262. https://doi.org/10.3390/nu13041262
5. Theoharides, T. C., Tsilioni, I., & Ren, H. (2019). Recent advances in our understanding of mast cell activation. Expert Review of Clinical Immunology, 15(6), 639-656. https://doi.org/10.1080/1744666X.2019.1596800
6. Afrin, L. B., Ackerley, M. B., Bluestein, L. S., et al. (2020). Diagnosis of mast cell activation syndrome: A global “consensus-2.” Diagnosis, 8(2), 137-152. https://doi.org/10.1515/dx-2020-0005
7. Weiler, C. R., Austen, K. F., Akin, C., et al. (2019). AAAAI Mast Cell Disorders Committee Work Group Report: Mast cell activation syndrome (MCAS) diagnosis and management. Journal of Allergy and Clinical Immunology, 144(4), 883-896. https://doi.org/10.1016/j.jaci.2019.08.023
8. American College of Medical Toxicology. (2025). Position statement: Medical toxicology considerations in the diagnosis and treatment of patients with concerns about mold-related inhalation exposures. https://www.acmt.net