Is It Perimenopause or Histamine? An Honest Answer
Here is what conventional medicine misses. You have been to the allergist, the gynecologist, maybe a cardiologist, and your labs came back normal every time. Nobody asked the one question that connects your worst week to your cycle. You feel flushed, your heart races at 3am, wine suddenly wrecks you, and it is always worse the week before your period. You are not imagining the pattern. You are noticing something real that your appointments were too short to catch. The honest version of this story is not the tidy loop you saw on Instagram, and it is not a dismissal either. There is a real, hormone-timed pattern here for some women. There is also a lot of certainty being sold that the science has not earned. In this piece I will show you where the pattern is real and where the mechanism runs out. Then I will give you one free four-week test that tells you more than a $300 lab ever will.
Is it perimenopause or is it histamine?
For some women it is both, working through the same overloaded clearance system, and almost no clinician connects them. Histamine is a signaling molecule your body makes and also takes in from food. It drives flushing, hives, headaches, a racing heart, and that wired-but-tired 3am wake-up. Perimenopause is the years-long hormonal swing before your last period. Estrogen does not glide down. It lurches up and crashes, sometimes within the same week.
Let me back up a little. Estrogen is one of your main sex hormones. In perimenopause it stops being predictable. When estrogen swings high, some women feel more reactive, more flushed, more itchy, more awake at the wrong hour. That overlap is exactly why nobody can tell you which one it is. The allergist does not ask about your cycle. The gynecologist does not ask about your skin.
The bottom line for you: “perimenopause or histamine” is the wrong question. For a subset of women, the two ride the same overloaded system at once. That does not mean the popular explanation is right. It means the pattern deserves a real look instead of a shrug.
Why hasn’t a doctor connected this for you?
Because the system is built to see one fragment at a time, and your symptoms live in the gaps between specialties. This is the 10-minute appointment problem. An allergist is trained to find an allergen. A gynecologist is trained to read your hormones. A cardiologist is trained to rule out the dangerous thing in your chest. None of them is trained, or paid, to sit with a woman and map her flushing against her menstrual calendar.
One woman I worked with had seen four allergists, two gynecologists, and a cardiologist across two years. Every visit ended with “your labs are normal.” Not one of them asked the question that finally cracked it open: when in your cycle does this happen? Her answer was immediate. The week before my period, every month, like clockwork.
That is the moment the picture changes. The naturopathic lens on this is not a different test. It is a different question. Instead of asking what the single broken part is, I ask a wider question. What is the pattern across your whole month, and what is your body trying to clear all at once.
What this means for the woman in front of me: the failure here is not in your body. It is in a system that never gave anyone the ten minutes to connect your cycle to your symptoms. The pattern was always there. It just needed someone to ask.
What does your liver actually do with estrogen and histamine?
Your body clears histamine mainly through two enzymes, and your liver and gut share the work of processing both histamine and estrogen. The first enzyme is DAO. DAO stands for diamine oxidase. Think of it as the bouncer at your gut wall, breaking down histamine from food before it gets into your bloodstream. The second is HNMT. HNMT stands for histamine N-methyltransferase. Think of it as the cleanup crew working inside your cells.
Both of those clearance routes can get overwhelmed. Picture a sink with a slow drain. If histamine pours in faster than DAO and HNMT can clear it, the sink backs up. That backed-up state is what people mean by a “histamine bucket” that is too full.
Now, estrogen runs through some of the same hepatic machinery. Hepatic just means liver-based. Your liver processes estrogen through a step called phase II conjugation. Phase II conjugation is the liver attaching a small tag to a molecule so your body can ship it out. The wellness claim is that estrogen and histamine compete for that shared liver capacity, so when one is high the other backs up.
Here is where I have to be honest with you. That competing-pathways idea is biochemically reasonable. It is not demonstrated in humans. The liver clearing both is plausible on paper. No study has shown that this specific traffic jam drives perimenopause symptoms in real women. I would rather tell you that than sell you a diagram that looks more certain than the data.
The bottom line for you: your gut and liver really do clear both histamine and estrogen, and that machinery really can get overwhelmed. The neat story that they fight over the same parking spot is a reasonable guess, not a proven fact.
A low-histamine diet cut symptoms in 18 patients while serum DAO failed to track it (Rentzos 2024).
Does estrogen really raise your histamine?
It can prime the cells that release histamine, but the strongest evidence for that comes from animal and laboratory studies, not from perimenopausal women. This is the part the wellness internet states like settled fact. I want to give you the real shape of it.
In the lab, estrogen does something interesting to mast cells. Mast cells are your immune system’s histamine grenades, packed with histamine and ready to release it when triggered. When researchers bathed mast cells in estradiol first, the cells released more histamine when triggered. Estradiol is the main, most potent form of estrogen. This is real, and it is repeatable.
Estradiol pre-incubation raised mast cell histamine release 2 to 3 fold in vitro (Cocchiara 1992).
Now the honest caveat, said in the same breath. That finding came from rat uterine tissue and human cells in a dish, not from women living through perimenopause. Estradiol alone did not even trigger release. It primed the cell, and something else pulled the trigger. So “estrogen raises your histamine” is too strong. “Estrogen may prime the cells that release histamine, mostly shown in animal and lab models” is the accurate sentence.
There is a second wrinkle most explainers leave out. One study found estrogen turning up a histamine-degrading enzyme rather than turning it down. In that tissue, estrogen helped clear histamine faster, the opposite of the popular loop. That single finding is why I do not trust the tidy diagram. The biology is messier than the arrows suggest, and any honest version has to hold both directions at once.
What this means for the woman in front of me: there is a believable reason your symptoms cluster when estrogen swings. That reason is mostly built on rats and test tubes. I will not dress up a maybe as a mechanism you can bank on.
Is “estrogen dominance” causing your symptoms?
This is the claim I will not make as fact, and the reason matters more than the slogan. “Estrogen dominance” is a popular wellness term for having too much estrogen relative to progesterone. It gives a name to real suffering, which is why it spreads. But it is loosely defined, and the causal chain behind it is not proven in human perimenopause.
The popular version goes like this. Estrogen dominance lowers your DAO, your liver stops clearing histamine, your symptoms flare, and a supplement stack fixes the loop. Every link in that chain is weaker than it sounds. The “estrogen lowers your DAO” step is contested, because one model showed estrogen doing the opposite. The “fix it with a stack” step has thin and partly industry-funded evidence.
Here is the root-cause version of this question, and it is not what the phrase “estrogen dominance” implies. The root cause is not a single villain hormone. It is total load against total clearance capacity. How much histamine is coming in from food, alcohol, and poor sleep. How well your gut and liver are clearing it. And your hormones swinging in the background. That framing is less catchy. It is also more true, and it points to things you can actually change.
The bottom line for you: I will not tell you estrogen dominance is causing your symptoms. The evidence does not let me say that honestly. I will tell you that load versus clearance is the frame that actually holds up.
So how do you find out cheaply if histamine is your driver?
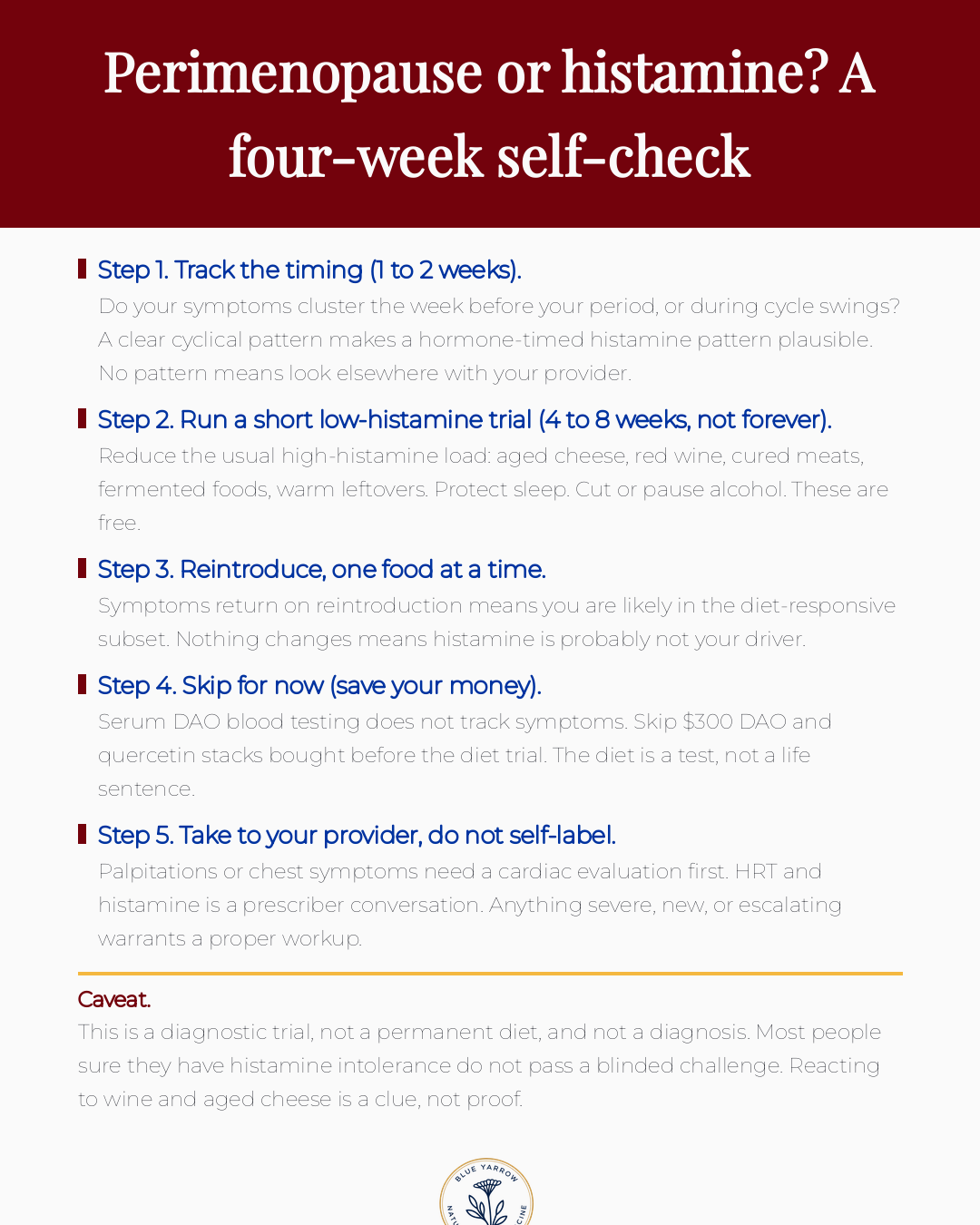
You run a free four-week experiment on yourself before you spend a dollar on testing. This is the most useful thing in the entire article, so I want to be specific. The single best diagnostic we have for this is not a lab. It is a structured low-histamine diet trial with reintroduction, run for four to eight weeks, never forever.
A low-histamine diet means temporarily reducing the heavy hitters. Aged cheese, red wine, cured and smoked meats, fermented foods, and leftovers stored warm. You also protect sleep and pause alcohol, because both raise the load. None of that costs money. All of it is reversible.
Then you reintroduce, one food at a time, and you watch. If symptoms return when you add the wine back, you likely belong to the diet-responsive group and you found your answer for free. If nothing changes across the whole trial, histamine is probably not your main driver. The kindest thing you can do then is stop restricting and look elsewhere with your provider.
I want to be blunt about what to skip. Skip the serum DAO blood test. Serum DAO is the level of that enzyme measured in your blood. It does not match the enzyme activity in your gut, and it does not track your symptoms. So it cannot answer the question you are paying it to answer. Skip the $300 DAO and quercetin stack bought before you have even run the diet trial. Quercetin is a plant compound often sold for histamine. The diet trial is cheaper, safer, and more informative than any of it.
What this means for the woman in front of me: you can get a real answer this month, for free, from your own kitchen. You do not have to hand $300 to a test that cannot tell you what you need to know.
Will HRT make your histamine symptoms worse?
Some women notice their histamine symptoms shift on HRT, and this is a conversation for your prescriber, not a decision to make from a blog. HRT stands for hormone replacement therapy, the prescribed estrogen and progesterone many women use in perimenopause. Because estrogen interacts with mast cells in the lab, it is biologically plausible that adding estrogen could change how reactive some women feel.
Plausible is not the same as predictable. Some women feel better on HRT. Some notice more reactivity. The route matters, and the formulation matters, and your individual history matters more than any general rule I could give you here. I am not going to advise you to start, stop, or change a dose. That is genuinely outside what public education should do, and it is your prescriber’s job.
What I will say is this. If you are weighing HRT and you also suspect histamine is part of your picture, bring both to the same appointment. Most women never get the chance to discuss them together, because the hormone conversation and the histamine conversation happen in two different offices. Putting them in one room is the whole point.
The bottom line for you: HRT and histamine can interact, and the direction varies woman to woman. The only safe place to sort it out is with the person who can actually prescribe and adjust.
What about the women who are sure they have this and don’t?
This is the caveat I refuse to bury, because it is the most honest and most useful thing I can give you. When researchers ran a blinded challenge, most people who were certain they had histamine intolerance did not actually react to histamine. A blinded challenge means you do not know whether you are getting histamine or a placebo, so your expectation cannot color the result.
A placebo-controlled challenge excluded histamine intolerance in 84.7% of suspected patients (JACI 2023).
Read that number again. In that study, histamine intolerance was excluded in roughly five of every six suspected patients. Many of them reacted to the placebo. That does not mean their suffering was fake. It means the body and the mind together can produce very real symptoms from expectation, and from the ordinary noise of perimenopausal life.
So why am I telling you this when it complicates everything? Because it is exactly why the cheap diet trial matters so much. Most self-diagnosis does not survive a blinded test. So the worst thing you can do is spend hundreds of dollars and commit to a restrictive life based on a guess. The diet trial is your own small, low-cost version of a test, and it can put you in the right group without the price tag.
What this means for the woman in front of me: reacting to wine and aged cheese is a clue, not a verdict. The goal is to find out cheaply which group you are actually in, instead of buying the label.
What I’d do this week
If you take one thing from this article, take this self-check and run it. It answers the question you came in with, “is it perimenopause or is it histamine,” and routes you to the lowest-cost first step. Save this. It is the whole article in one screen.
The honest place to land
You came here asking whether your worst weeks are perimenopause or histamine. The most truthful answer I can give you is that for some women it is both. The two ride the same overloaded clearance system. And you can find out which group you are in for the price of groceries you already buy.
I am not going to hand you a tidy loop and a supplement stack, because the science does not back that. You deserve better than confident-sounding fiction. The pattern is real. The mechanism is mostly rats and test tubes for now. The test is your own kitchen. That is the whole honest picture, and it is enough to act on this week.
This is Part 1 of a three-part series on perimenopause and histamine. The next piece goes deeper into mast cells and the specific signals behind the flush. For now, I want to leave you with one question. When you map your symptoms against your cycle this month, what pattern shows up that nobody ever asked you about?
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Frequently asked questions
Is it perimenopause or histamine? For some women it is both at once, which is why no single specialist connects it. Perimenopausal estrogen swings can prime histamine release, mostly shown in lab studies. The fastest honest way to tell is a four-week low-histamine diet trial with reintroduction, run before you spend money on testing.
Will HRT make it worse? It might shift your symptoms in either direction, and this is genuinely individual. Estrogen interacts with mast cells in the lab, so adding it could change reactivity for some women and help others. Do not start, stop, or change a dose based on a blog. Bring the hormone question and the histamine question to your prescriber together.
Do I need a DAO supplement? Not as a first step, and probably not before a diet trial. The evidence for DAO supplements is limited and partly funded by the companies that sell them. They are symptomatic at best and do not fix any hormonal driver. Run the free diet trial first, then talk to your provider about whether a supplement adds anything.
Why did this start in my late 30s? Because that is often when progesterone begins falling and estrogen starts swinging instead of cycling smoothly. That hormonal turbulence is one plausible reason previously tolerated foods and triggers suddenly feel different. The onset is real even though conventional care rarely names it. Tracking your timing for a month usually makes the new pattern visible.
Should I do a low-histamine diet forever? No. It is a four-to-eight-week diagnostic trial, not a way of life. Prolonged restriction risks nutritional gaps and a difficult relationship with food, especially in midlife. The whole point of reintroduction is to find your real triggers and return everything else to your plate. If the diet helps, narrow it to what actually matters, then stop restricting the rest.
Should I get my DAO levels tested? A blood test for DAO will not give you a reliable answer. Serum DAO does not match the enzyme activity in your gut, and it varies day to day. It cannot tell you whether histamine is your driver. Save the money and run the diet trial instead. It is cheaper and more informative than the lab.
References
1. Cocchiara, R., Albeggiani, G., Di Trapani, G., et al. (1992). Oestradiol enhances in vitro the histamine release induced by embryonic histamine-releasing factor from uterine mast cells. Human Reproduction, 7(8), 1036-1041. https://doi.org/10.1093/oxfordjournals.humrep.a137790
2. Comas-Baste, O., Sanchez-Perez, S., Veciana-Nogues, M. T., et al. (2020). Histamine intolerance: The current state of the art. Biomolecules, 10(8), 1181. https://doi.org/10.3390/biom10081181
3. Ford, A. C., Staudacher, H. M., & Talley, N. J. (2024). Postprandial symptoms in disorders of gut-brain interaction. Gut, 73(7), 1199-1211. https://doi.org/10.1136/gutjnl-2023-331833
4. Hrubisko, M., Danis, R., Huorka, M., & Wawruch, M. (2021). Histamine intolerance, the more we know the less we know. A review. Nutrients, 13(7), 2228. https://doi.org/10.3390/nu13072228
5. Jensen, F., Woudwyk, M., Teles, A., et al. (2010). Estradiol and progesterone regulate the migration of mast cells from the periphery to the uterus and induce their maturation and degranulation. PLoS One, 5(12), e14409. https://doi.org/10.1371/journal.pone.0014409
6. Liang, X. H., Zhao, Z. A., Deng, W. B., et al. (2010). Estrogen regulates amiloride-binding protein 1 through C/EBP-beta in mouse uterus during embryo implantation and decidualization. Endocrinology, 151(10), 5007-5016. https://doi.org/10.1210/en.2010-0170
7. Rentzos, G., Weisheit, A., Ekerljung, L., & van Odijk, J. (2024). Measurement of diamine oxidase during low-histamine or ordinary diet in patients with histamine intolerance. European Journal of Clinical Nutrition, 78(8), 726-731. https://doi.org/10.1038/s41430-024-01448-2
8. Ridolo, E., Incorvaia, C., Martignago, I., et al. (2019). Sex in respiratory and skin allergies. Clinical Reviews in Allergy & Immunology, 56(3), 322-332. https://doi.org/10.1007/s12016-017-8661-0
9. Schnedl, W. J., & Enko, D. (2021). Histamine intolerance originates in the gut. Nutrients, 13(4), 1262. https://doi.org/10.3390/nu13041262