Why Perimenopause Hives Aren’t a Histamine Problem
If you were fine with wine until you weren’t, this is for you. One glass now leaves you flushed and itchy. Aged cheese gives you hives. The week before your period, your whole body feels like it turned against you, and your hot flashes arrived at the same time. Your doctor ran labs, called them normal, and offered an antihistamine or an SSRI. Meanwhile the internet told you estrogen dominance is flooding you with histamine. You probably have MCAS, it said, and stacking Pepcid and Claritin will fix it. Both of those answers miss the same thing. The actor here is not histamine on its own. It is a specific immune cell called the mast cell. It sends one signal that tells us which of your symptoms an antihistamine might actually touch and which it never will. That single distinction is what this whole post is built around. By the end you will know which symptom belongs to which mechanism, and what to do this week.
The short version: some of your symptoms are genuinely histamine-related, your hot flashes are not, and a symptom checklist online is not a diagnosis.
Why is my body suddenly reacting to wine, cheese, and heat in my forties?
Because perimenopause changes the cells that decide how reactive your body is. The timing makes it feel sudden even when the setup was years in the making. Here is what conventional medicine misses. It treats your hives and your hot flashes as two unrelated complaints and hands you one pill for each. It never asks whether a single shift underneath both could explain why they showed up the same season. The naturopathic lens on this starts at that shared root, not at the prescription pad.
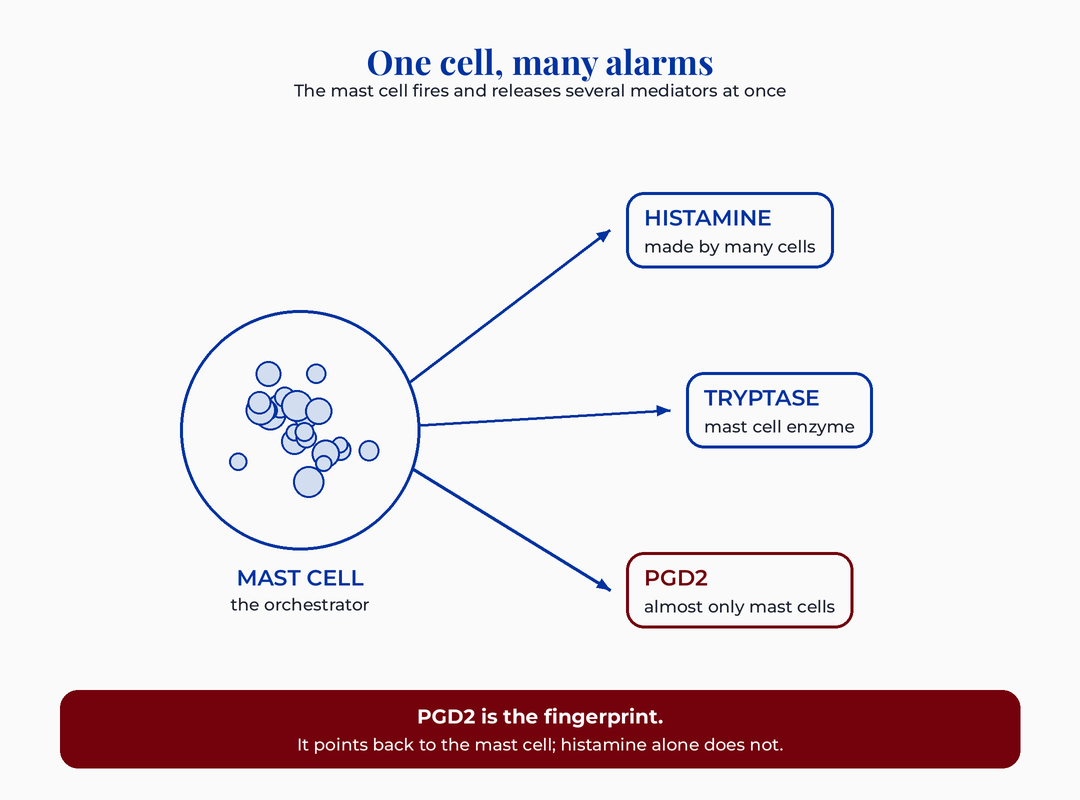
Let me back up and name the cell. A mast cell is an immune cell that sits in your skin, your gut lining, your airways, and around your blood vessels. Think of it as a tripwire packed with chemical alarms. When something trips it, it releases its contents in a burst. That burst is called degranulation. One of the alarms it releases is histamine, the molecule behind the itch, the flush, and the runny nose you already know.
Here is where the popular story gets the biology half right and half wrong. Histamine is real and it does drive some of what you feel. But many different cells in your body make histamine, which makes it a noisy, nonspecific signal. The mast cell is the orchestrator, and it releases far more than histamine when it fires. PGD2 comes almost entirely from mast cells, which makes it far more specific than histamine (Roberts 1991). PGD2 is short for prostaglandin D2. It is another chemical alarm the mast cell sends. Because almost nothing else in the body makes it, finding PGD2 is a fingerprint that points back to the mast cell specifically.
So the reframe is this. You do not have a histamine problem in the loose way the internet means it. You have a mast cell that has become easier to trip. What this means for the woman reading this: the question is not how to block histamine. It is why your mast cell is firing more easily now, and which of your symptoms that actually explains. That is the root-cause version of this question, and it changes the answer.
What does estrogen have to do with my mast cells?
Estrogen can prime mast cells to fire more easily, but most of that proof is still in mice and lab dishes, not in women. I want to be honest about the strength of this evidence, because the wellness internet states it as settled fact and it is not.
Here is what the research actually shows. Mast cells carry receptors for estrogen on their surface. When estradiol, the main form of estrogen, binds those receptors, it can nudge the cell toward degranulation. That part is biologically real. The catch is that most of this work was done in animals and in cell cultures, not in perimenopausal women living their lives. So the mechanism is plausible and partly demonstrated, but the human causal step is thin. I share that gap on purpose. A doctor who admits the human proof is still mostly mice and dishes is one you can trust on her next claim too.
There is a second thread worth knowing. Estrogen also appears to lower the activity of an enzyme called DAO. DAO, or diamine oxidase, is the enzyme that breaks histamine down in your gut after you eat. If estrogen reduces DAO, histamine from food and wine clears more slowly, and you feel it longer. This comes from the histamine-intolerance research, not from perimenopause studies specifically, so I hold it loosely. It does help explain the pattern so many women describe.
That pattern is the “worse the week before my period” complaint. During the perimenopause transition, estradiol does not glide downward. It swings, sometimes higher than it ever was, then crashes. Those swings are exactly the kind of input that could prime a mast cell and slow histamine clearance at the same time. The naturopathic read: your symptoms are not random, they track a hormonal rhythm. That rhythm is the lever worth understanding before anyone reaches for a pill.
Micro-summary so far: the mast cell is the actor, and PGD2 is its specific fingerprint. Estrogen can make the cell more reactive, though the strongest human proof is still missing.
Will antihistamines fix my hot flashes?
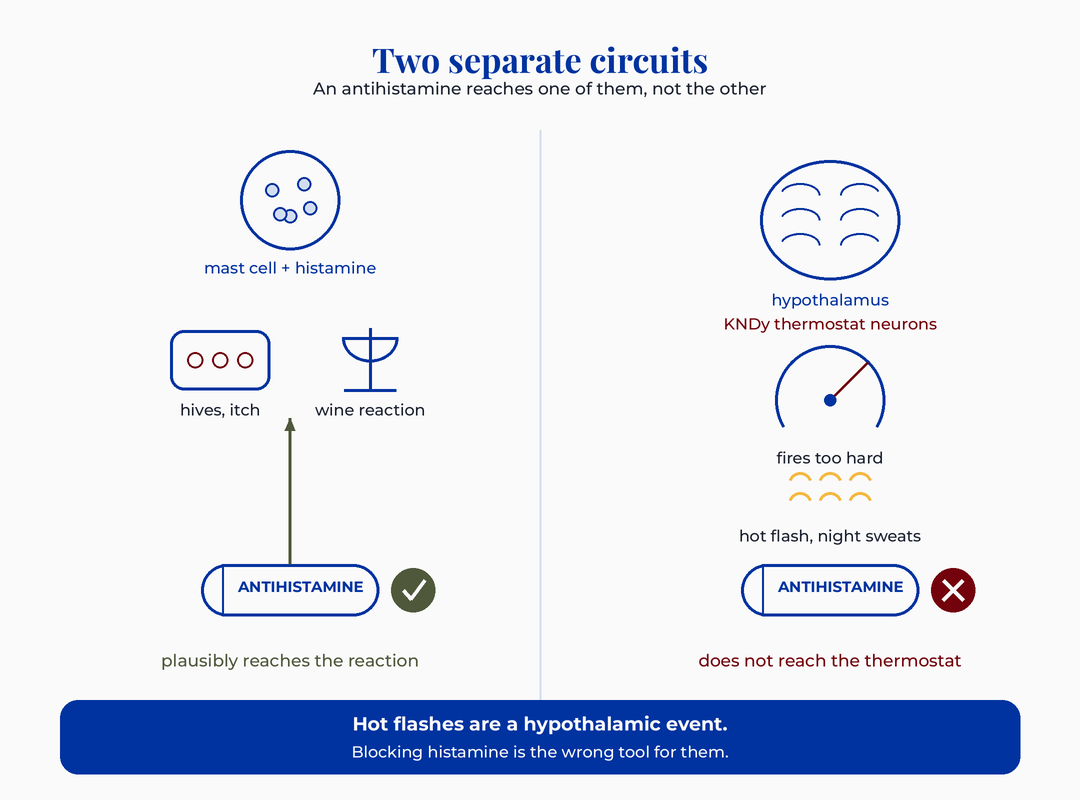
No, and this is the single most important correction in this entire post. Your hot flashes do not come from histamine, so a medication that blocks histamine is not built to touch them. Conventional medicine actually gets this part right, but it rarely explains it to you, and the wellness internet gets it flat wrong.
Let me explain where a hot flash actually comes from. Deep in your brain sits the hypothalamus, your body’s thermostat. Near it is a cluster of cells called KNDy neurons. KNDy neurons are a small group of brain cells that help set your internal temperature. Plain version: they are the dial on the thermostat. When estrogen is steady, it keeps these neurons calm. When estrogen falls in perimenopause, that calming restraint lifts, the neurons fire too hard, and your brain mistakenly decides you are overheating. So it dumps heat the only ways it knows: it flushes your skin and makes you sweat. That is a hot flash. A hot flash is also called a vasomotor symptom, meaning a symptom of blood vessels opening to release heat.
Hot flashes come from hypothalamic KNDy neurons, not histamine, so antihistamines cannot fix them (Gombert-Labedens 2025). This is why the newest targeted hot flash drug, fezolinetant, works on that KNDy circuit and not on histamine at all. It is also why the proven non-hormonal options, certain SSRIs and SNRIs, work through brain chemistry rather than the immune system.
I want to be fair to the open question here, because honesty cuts both ways. Histamine is also a brain chemical that plays a role in temperature and sleep. So I will not claim an antihistamine does absolutely nothing centrally. What I will say is firm. The hot flash itself is a hypothalamic event, and antihistamines are not a proven hot flash treatment. The women who report relief are very likely catching the high placebo response that vasomotor symptoms are famous for. What this means for the woman in front of me: if a hot flash is your main complaint, an antihistamine is the wrong tool. Reaching for it can delay the conversation about therapies that actually target the circuit.
Consider a woman I have seen described in cases I’ve reviewed. Forty-three, new wine intolerance, new hives, and hot flashes that wake her at 3am. She found the Pepcid-and-Claritin trend, felt some relief from the skin reactions, and assumed it was working on everything. The flashes never budged. She spent four months thinking she was failing the protocol. She was not failing anything. The protocol was simply never going to reach the part of her brain generating the flash.
Do I have MCAS, or histamine intolerance, or is it just hormones?
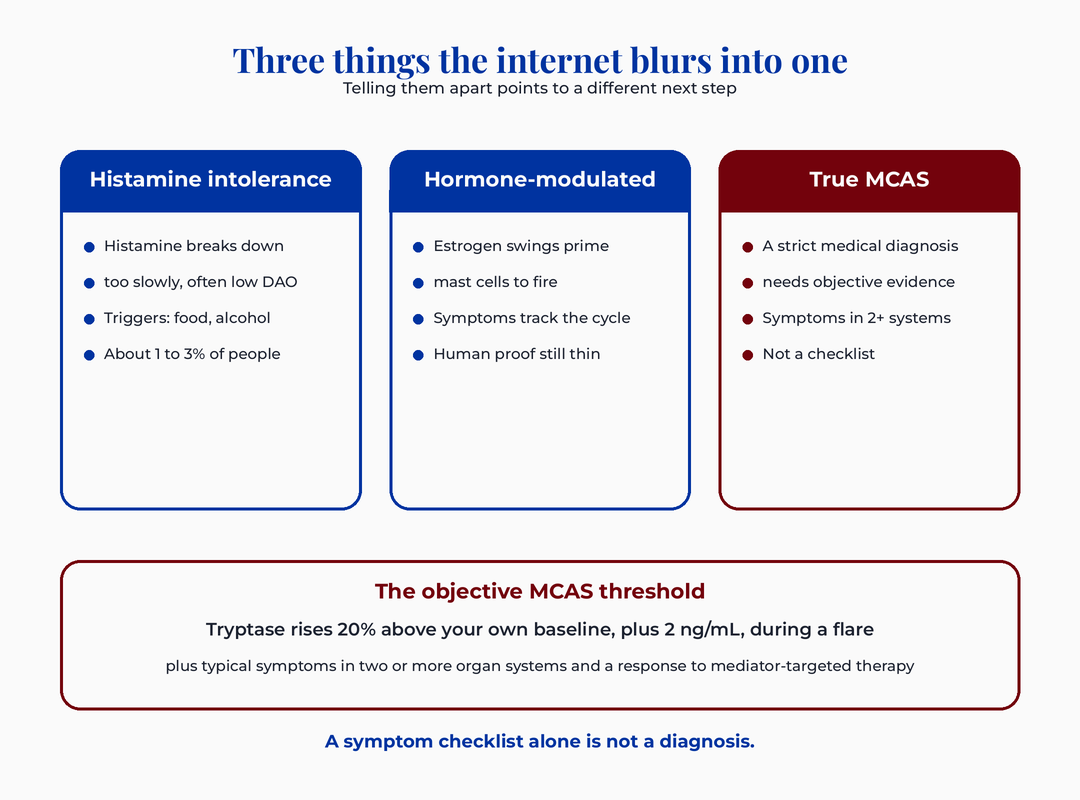
Most likely it is hormone-modulated reactivity, sometimes histamine intolerance, and only rarely true MCAS, and the three are not the same thing. The internet blurs them into one scary label. Drawing the line is where a doctor earns her keep, so let me draw it cleanly.
Histamine intolerance
This means your body breaks histamine down too slowly, often because DAO activity is low. Food and alcohol are the usual triggers. It affects a small slice of people, somewhere around 1 to 3 percent in the research. It is a real construct, though even the experts admit the diagnostic standards are still loose. If wine, aged cheese, and fermented foods are your reliable triggers, this is a reasonable lens.
Hormone-modulated mast cell reactivity
This is the perimenopause-specific version. Estrogen swings prime your mast cells so they fire more easily, and your symptoms rise and fall with your cycle. The mechanism is real but the human evidence is still mostly mice and dishes, as I said earlier. This is probably the bucket most of the women reading this fall into, and it is the one the research community has studied the least.
True MCAS
MCAS stands for mast cell activation syndrome. This is a genuine medical diagnosis, and it has strict criteria. Tryptase is a chemical the mast cell releases that doctors can measure in your blood. The consensus requires an objective rise in tryptase during a flare, specifically 20 percent above your own baseline plus 2 ng/mL. It also requires typical symptoms in two or more organ systems and a response to mediator-targeted treatment. The broad online MCAS criteria show low diagnostic specificity and attach the label to unrelated conditions (Solomon 2024). A symptom checklist by itself is not a diagnosis, no matter how many of the boxes you tick.
You may have seen the claim that MCAS affects up to 17 percent of people. Hold that number loosely. It comes from one camp inside the field and is contested by the mainstream consensus. The broad criteria behind it are exactly the ones shown to be imprecise.
Micro-summary: histamine intolerance is a clearance problem, and hormone-modulated reactivity is the perimenopause pattern. True MCAS is a strict diagnosis that a checklist cannot give you. Telling them apart matters because each points to a different next step.
If antihistamines help, doesn’t that prove I have MCAS?
No. Feeling better on an antihistamine tells you that some of your symptoms involve histamine. It does not confirm a diagnosis, and it does not work backward into MCAS. This is one of the most common logic traps in the whole conversation, so it is worth slowing down on.
Symptom response to a mediator-blocking drug is only one of several criteria for MCAS, and it is never enough on its own. Plenty of things improve on an antihistamine without anyone having MCAS. Seasonal allergies do. Ordinary hives do. And the placebo effect is powerful, especially with symptoms that wax and wane on their own. When something naturally comes and goes, any treatment you start during a bad week will look like it worked when the good week arrives. That is regression to the mean, not proof.
Here is the part I find genuinely useful to know. An antihistamine plausibly eases the histamine-driven reactions, the itching, the hives, some food and alcohol responses, and for some women certain headaches. That is a fair use of the tool. What it cannot do is tell you why your mast cells got reactive, treat your hot flashes, or diagnose a syndrome.
What this means for you: relief is information, not a verdict, and it is worth bringing to a real workup rather than a self-label.
Think of a second woman from cases I’ve reviewed. She had read that antihistamine relief equals MCAS, so she arrived convinced she had a rare immune disease and braced for a frightening future. Her actual picture was cyclical, hormone-linked reactivity plus garden-variety histamine sensitivity to wine. The relief was real. The label was wrong. Unwinding the fear took longer than explaining the biology, which tells you something about how much the framing online costs women emotionally.
What about a low-histamine diet, and will HRT help or hurt?
A low-histamine diet can reduce the food-and-alcohol portion of your symptoms. It also carries a real risk of slipping into over-restriction, so it needs structure rather than fear. HRT is genuinely individual, and the honest answer is that it can move histamine symptoms in either direction depending on the person.
On diet first. Lowering high-histamine foods, aged cheese, cured meats, fermented foods, and alcohol, can ease the reactions that run through histamine. The trap is that these diets sprawl, the lists online get longer every year, and women end up afraid of food. The gastroenterology guidance is explicit that elimination diets need nutritional guidance to avoid that harm. A short, structured trial with a clear endpoint beats an open-ended restriction every time. This is the same anti-orthorexia stance the chronic disease pillar holds elsewhere.
On HRT. Because estrogen interacts with mast cells and with DAO, smoothing out the wild swings of perimenopause can settle symptoms for some women. For others, adding estrogen seems to stir reactivity up, at least at first. There is no clean rule here, and anyone who gives you one is overselling. Have this conversation with a provider who adjusts based on how your body actually responds. It is not a decision to make from a social media post.
Micro-summary: diet helps the food-driven slice if you keep it structured. HRT is a real option that has to be personalized rather than prescribed by trend.
What I’d do this week
Before anything else, get oriented. Most women in this position are carrying three different mechanisms under one scary label, and sorting them is the first relief. The card below is the tool I would want in your hands. Screenshot it, save it, and bring it to your next appointment.
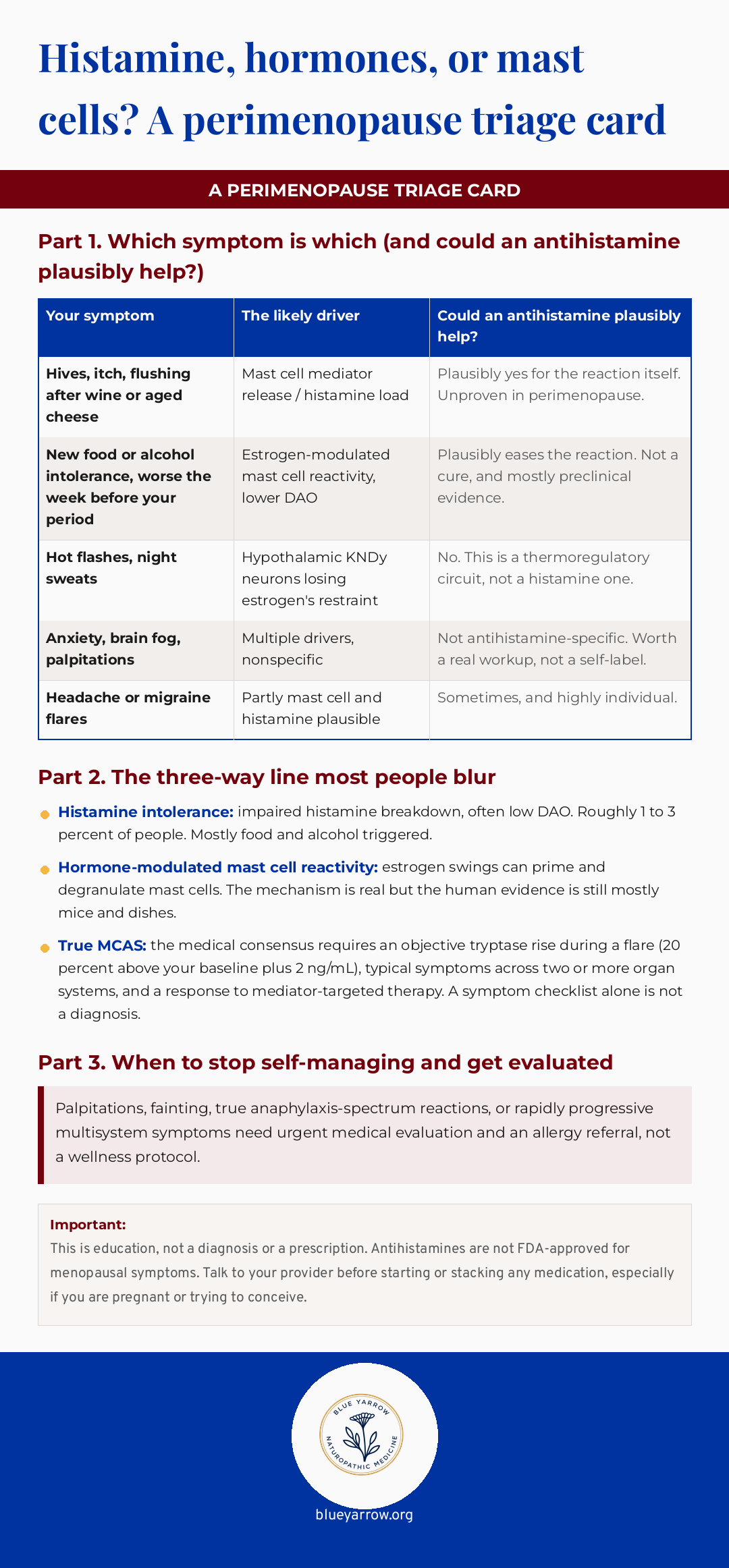
Beyond the card, three steps for the week. First, track for seven days. Write down each symptom, what preceded it, and where you are in your cycle. Patterns surface fast when you put them on paper. Second, run one structured experiment, not five. If wine and aged cheese are your clear triggers, trial a lower-histamine week with a defined endpoint. Notice what changes and what does not. Third, separate your symptoms into the card’s buckets before you decide anything. The hot flashes go in their own column, and they get their own conversation.
This topic is Part 2 of a three-part series on histamine in perimenopause. Part 1 covers how estrogen and histamine clearance interact in the liver. Part 3 covers the environmental and mold-driven side of histamine load.
So here is my question for you. When your symptoms flare, which column of that card do they actually land in? And have you been treating all of them as if they were the same thing?
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Frequently asked questions
Should I take Pepcid and Claritin for my perimenopause symptoms? That combination may ease histamine-driven reactions like hives or wine intolerance for some women, but no clinical trial has tested it in perimenopause, and it will not touch hot flashes. Antihistamines are not FDA-approved for menopausal symptoms. Talk to your provider before starting or stacking any medication.
Is estrogen dominance causing my histamine problems? The estrogen-mast cell and estrogen-DAO links are real, but most of the proof is preclinical, in animals and lab dishes. “Estrogen dominance” is a loosely defined wellness term, not a measured clinical state in perimenopause. Your symptoms more likely track estrogen’s swings, not a single fixed excess.
Will HRT make my histamine symptoms better or worse? It depends on the person, and that is the honest answer. Smoothing out perimenopause’s estrogen swings settles symptoms for some women and stirs reactivity up for others, at least initially. There is no universal rule. This is a decision to personalize with a provider who adjusts based on your response.
Is a low-histamine diet worth it, or is that just orthorexia? A short, structured low-histamine trial can reduce food-and-alcohol-driven symptoms. The risk is real that it sprawls into fearful over-restriction. Gastroenterology guidance recommends nutritional support for elimination diets. Keep it time-limited with a clear endpoint rather than open-ended.
How do I know if I actually have MCAS? True mast cell activation syndrome requires objective evidence, not a checklist. The consensus needs a measured tryptase rise during a flare, symptoms across two or more organ systems, and a response to mediator-targeted therapy. The broad online criteria have low diagnostic specificity. An allergy or mast cell specialist can evaluate properly.
Why are my symptoms worse the week before my period? Estradiol swings hard in perimenopause, and those swings can prime mast cells to fire more easily while also slowing histamine breakdown through lower DAO activity. Your reactivity rises and falls with your hormonal rhythm, which is why the days before your period feel like the worst of it.
References
1. Roberts, L. J., & Oates, J. A. (1991). Biochemical diagnosis of systemic mast cell disorders. Journal of Investigative Dermatology, 96(3 Suppl), 19S-24S. https://doi.org/10.1111/1523-1747.ep12468945
2. Frieri, M. (2018). Mast cell activation syndrome. Clinical Reviews in Allergy & Immunology, 54(3), 353-365. https://doi.org/10.1007/s12016-015-8487-6
3. Loewendorf, A. I., Matynia, A., Saribekyan, H., Gross, N., Csete, M., & Harrington, M. (2016). Roads less traveled: Sexual dimorphism and mast cell contributions to migraine pathology. Frontiers in Immunology, 7, 140. https://doi.org/10.3389/fimmu.2016.00140
4. Gombert-Labedens, M., Vesterdorf, K., Fuller, A., Maloney, S. K., & Baker, F. C. (2025). Effects of menopause on temperature regulation. Temperature, 12(2), 92-132. https://doi.org/10.1080/23328940.2025.2484499
5. Pertynska-Marczewska, M., & Pertynski, T. (2024). Non-hormonal pharmacological interventions for managing vasomotor symptoms: How can we help, 2024 landscape. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 302, 141-148. https://doi.org/10.1016/j.ejogrb.2024.09.013
6. Comas-Baste, O., Sanchez-Perez, S., Veciana-Nogues, M. T., Latorre-Moratalla, M., & Vidal-Carou, M. C. (2020). Histamine intolerance: The current state of the art. Biomolecules, 10(8), 1181. https://doi.org/10.3390/biom10081181
7. Gulen, T. (2024). Using the right criteria for MCAS. Current Allergy and Asthma Reports, 24(2), 39-51. https://doi.org/10.1007/s11882-024-01126-0
8. Solomon, B. D., & Khatri, P. (2024). Clustering of clinical symptoms using large language models reveals low diagnostic specificity of proposed alternatives to consensus mast cell activation syndrome criteria. The Journal of Allergy and Clinical Immunology, 155(1), 213-218.e4. https://doi.org/10.1016/j.jaci.2024.09.006
9. Aziz, Q., Harris, L. A., Goodman, B. P., Simren, M., & Shin, A. (2025). AGA clinical practice update on GI manifestations and autonomic or immune dysfunction in hypermobile Ehlers-Danlos syndrome: Expert review. Clinical Gastroenterology and Hepatology, 23(8), 1291-1302. https://doi.org/10.1016/j.cgh.2025.02.015