Your Blood Count Is Normal. So Why Are You Exhausted?
If your bloodwork came back “normal” but you are still dragging yourself through the day, your doctor may have checked the wrong number. A standard blood count can read perfectly normal while your iron stores sit nearly empty, because your body quietly drains its reserves to keep your circulating blood in range. I am Dr. Shad Abdulla, ND, and I want to walk you through the number almost no one orders, what the evidence honestly says iron can and cannot do for your fatigue, and how to act on it without falling for the wellness-feed version. You were not imagining this.
Tired woman holding a normal lab printout while her ferritin sits low, illustrating iron deficiency missed by a standard blood count
What conventional medicine misses about “normal” iron
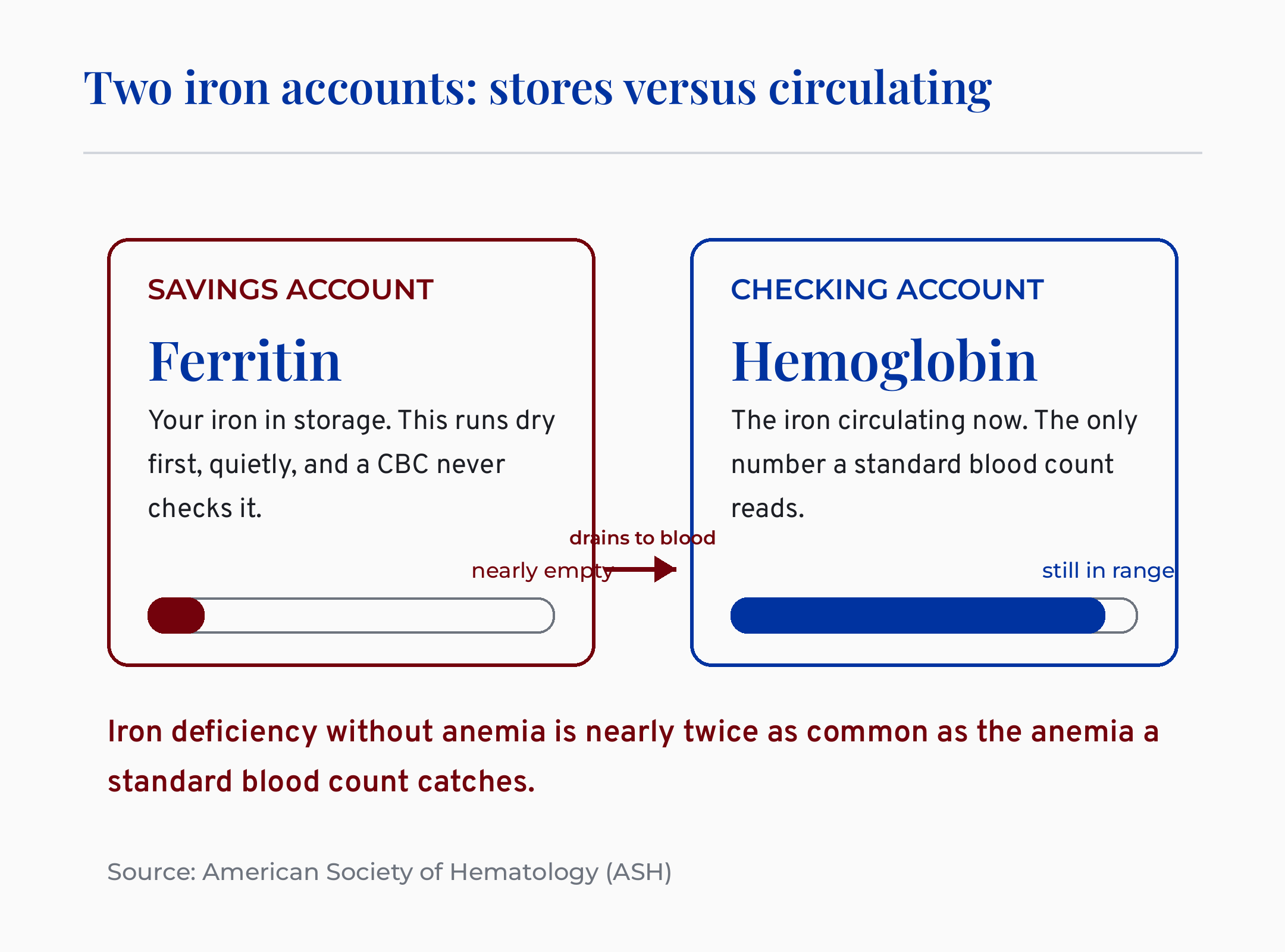
Here is what conventional medicine misses here. A complete blood count checks your hemoglobin, meaning the iron actively circulating in your blood right now. It does not check ferritin, meaning the iron your body has in storage. So the test that gets ordered measures your checking account while your savings account quietly runs dry.
This is the diagnostic miss at the heart of this whole conversation. Your body protects hemoglobin at all costs. When iron gets scarce, it pulls from storage first and keeps your circulating blood looking fine for a long time. That is why you can feel wrung out for a year while every blood count comes back unremarkable.
Iron deficiency without anemia is nearly twice as common as the anemia a standard blood count catches. That figure comes from the American Society of Hematology, and it reframes the whole problem. The version of low iron that shows up on a CBC is the smaller, later stage. The version that gets dismissed is the more common one.
What this means for the woman reading this: if you were told you are fine because your CBC was normal, you were handed a true answer to the wrong question. The right question needed a different test.
What number should I actually ask for instead of a CBC?
Ask for ferritin, your iron stores, not just a CBC. Ferritin is the single number that catches deficiency while a blood count still reads normal. Without it, early iron depletion is essentially invisible to the standard panel.
Ferritin is not a perfect number, and you deserve to know why. It is also an inflammation marker. When your body is fighting something, ferritin can climb and mask a real deficiency. So a “normal” ferritin during an infection or a flare can still hide empty stores underneath.
That is why I read ferritin alongside two other numbers, not in isolation. Transferrin saturation tells you how much iron is actually riding around available for use. CRP, meaning C-reactive protein, is a simple inflammation marker that tells you whether your ferritin reading can be trusted at face value.
In cases I have reviewed, this trio is what separates a confident answer from a guess. Ferritin alone can mislead. Ferritin read next to transferrin saturation and CRP rarely does.
What this means for you: when you ask, ask for all three. “Can we check my ferritin, transferrin saturation, and CRP, not just my CBC?” That one sentence changes the appointment.
How low is low? The ferritin number debate, honestly
Under about 30 micrograms per liter is deficient by most guidelines. Between 30 and 50 with fatigue and a normal blood count is the zone most worth acting on. Over 100 mainly rules deficiency out rather than confirming you are optimized.
Now, the honest part. The exact cutoff is genuinely contested, and I am not going to pretend it is settled. The American Society of Hematology has openly argued that female ferritin reference ranges were set too low to begin with. Different specialties draw the line at 15, at 25, at 30, at 50.
So what do you do with disagreement? You use the threshold that the actual fatigue trials used. The landmark study in this space enrolled women with ferritin below 50 and a normal blood count, then tested whether iron helped. That makes “below 50 with fatigue” a reasonable action zone, not a hard law of nature.
Here is the trap on the other side. The wellness feed has decided everyone needs ferritin over 100, and that is an overreach. The over-100 figure earns its keep in specific situations, like restless legs or confirming you are fully repleted. It is not a universal target to chase.
The naturopathic lens on this is not a fixed magic number, it is a moving target read in context. Your ferritin gets interpreted next to your symptoms, your inflammation, and your bleeding pattern, not against a one-size number from an Instagram caption.
Does iron actually fix the fatigue, or is that hype?
Here is the most honest answer you will read on this topic. In women with fatigue, a normal blood count, and low ferritin, iron produces a modest but real drop in how tired they feel. It is worth doing. It is also not the miracle the supplement aisle promises.
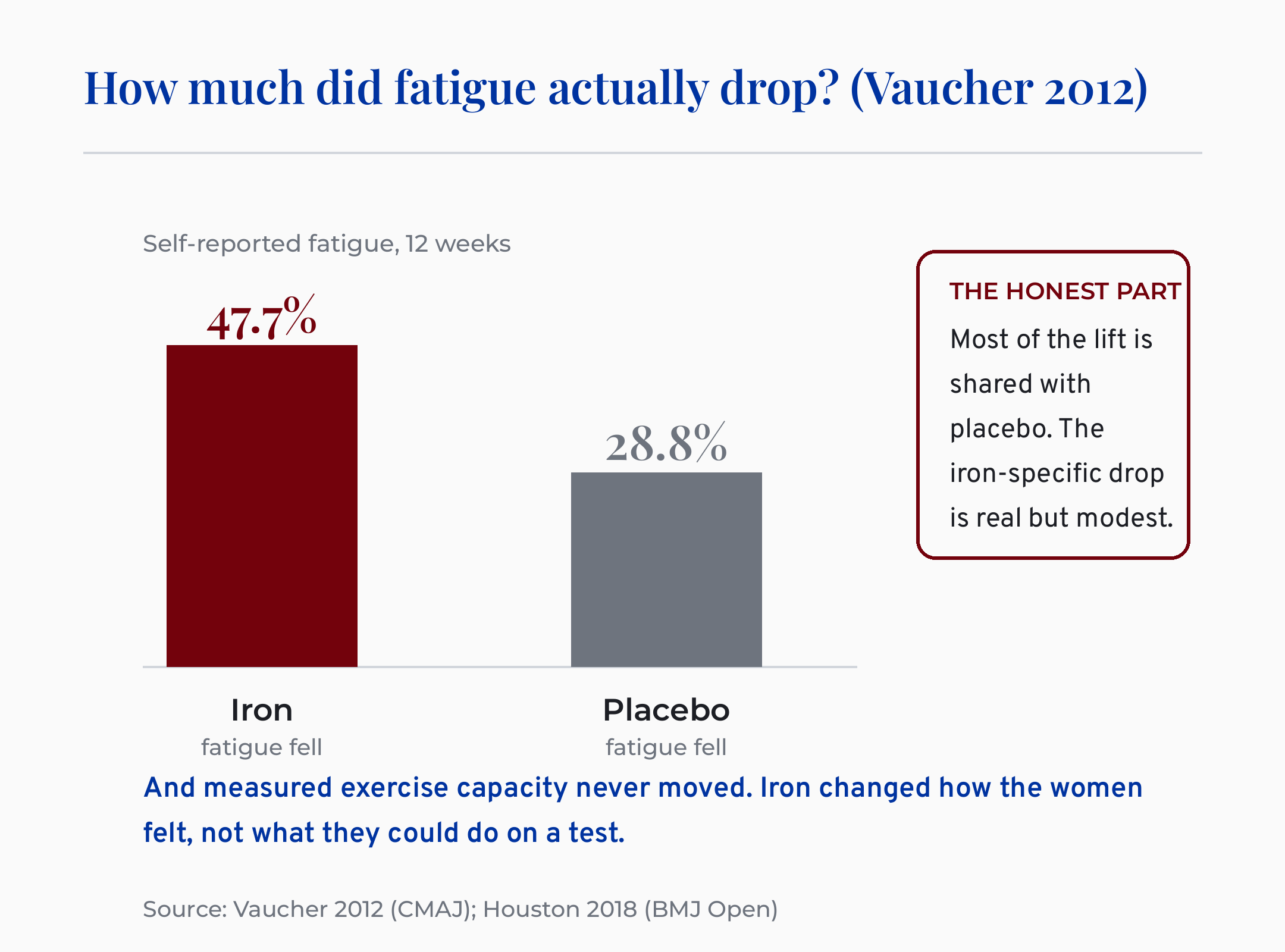
Let me show you the actual study rather than a compressed citation. Researchers gave non-anemic women with low ferritin either iron or a placebo for twelve weeks, then measured their fatigue. The iron group’s fatigue fell about 48 percent. The placebo group’s fatigue fell about 29 percent on its own.
Sit with that placebo number for a second. Iron cut fatigue 48% versus 29% on placebo, but measured exercise capacity never moved. Most of what women feel on iron is real, and a large share of it is also shared with sugar pills. The iron-specific bump is genuine but modest.
And the performance piece matters. When researchers pooled eighteen trials, iron reduced self-reported fatigue but did not improve objective physical capacity. Your treadmill time, your oxygen uptake, your measured strength did not climb. Iron changed how the women felt, not what they could do on a test.
I know that sounds like I am talking you out of the thing you came here for. I am not. A modest, real, low-risk improvement in how you feel through your day is a legitimate win. Naming the placebo and the performance ceiling honestly is exactly what separates a clinician from a creator selling you a fix.
What this means for the woman in front of me: if your ferritin is low and you are exhausted, repleting iron is reasonable and may genuinely help you feel better. Just do not expect it to turn you into an athlete or to be your whole answer.
Why is my iron low in the first place? (the part that actually matters)
Low iron is a sign, not a final diagnosis. The real question is not “how do I refill it” but “why am I losing it.” Refilling the tank without finding the leak means you are back here in six months.
This is the root cause of the whole thing, and it is the part the symptom-list content skips. Low ferritin is a symptom, and the real diagnosis is why you are losing iron, not the empty number itself. That distinction is the difference between a patch and a fix.
The common drivers cluster by life stage. For women in their thirties, it is often heavy periods or postpartum depletion. Many tell me a version of “I thought this was just being a tired mom.” It frequently was not just that.
For women moving into their forties, perimenopause changes the picture. Periods can get heavier and more frequent before they taper, and that shift can quietly drain iron faster than your diet can replace it. Your changing cycle can be the leak.
Other drivers sit in the gut. Celiac disease and poor absorption can starve you of iron even on a good diet. Slow blood loss from the digestive tract can do it silently. This is the root-cause version of this question, and it is why a thoughtful workup beats a blind supplement.
Some findings need a real workup, not a supplement. Blood in your stool, unexplained weight loss, or iron deficiency with no menstrual cause to explain it all warrant investigation, not reassurance. Those are the red flags that send you back to your doctor, not to the supplement aisle.
In my naturopathic training, the discipline that stuck with me was refusing to just refill iron without hunting for the leak. Patients I have worked with were sometimes surprised that the more important conversation was about their cycle or their gut, not the brand of iron.
What this means for you: when your ferritin comes back low, the next sentence out of your mouth should be a question. “If my ferritin is low, what is causing me to lose iron?”
If I supplement, how do I take iron so it actually absorbs?
Most people take iron in a way that absorbs less and hurts more. The smarter, better-studied approach is to take it every other day, as a single morning dose, with vitamin C. It absorbs more total iron and is gentler on your gut than the daily divided dosing most people are told to use.
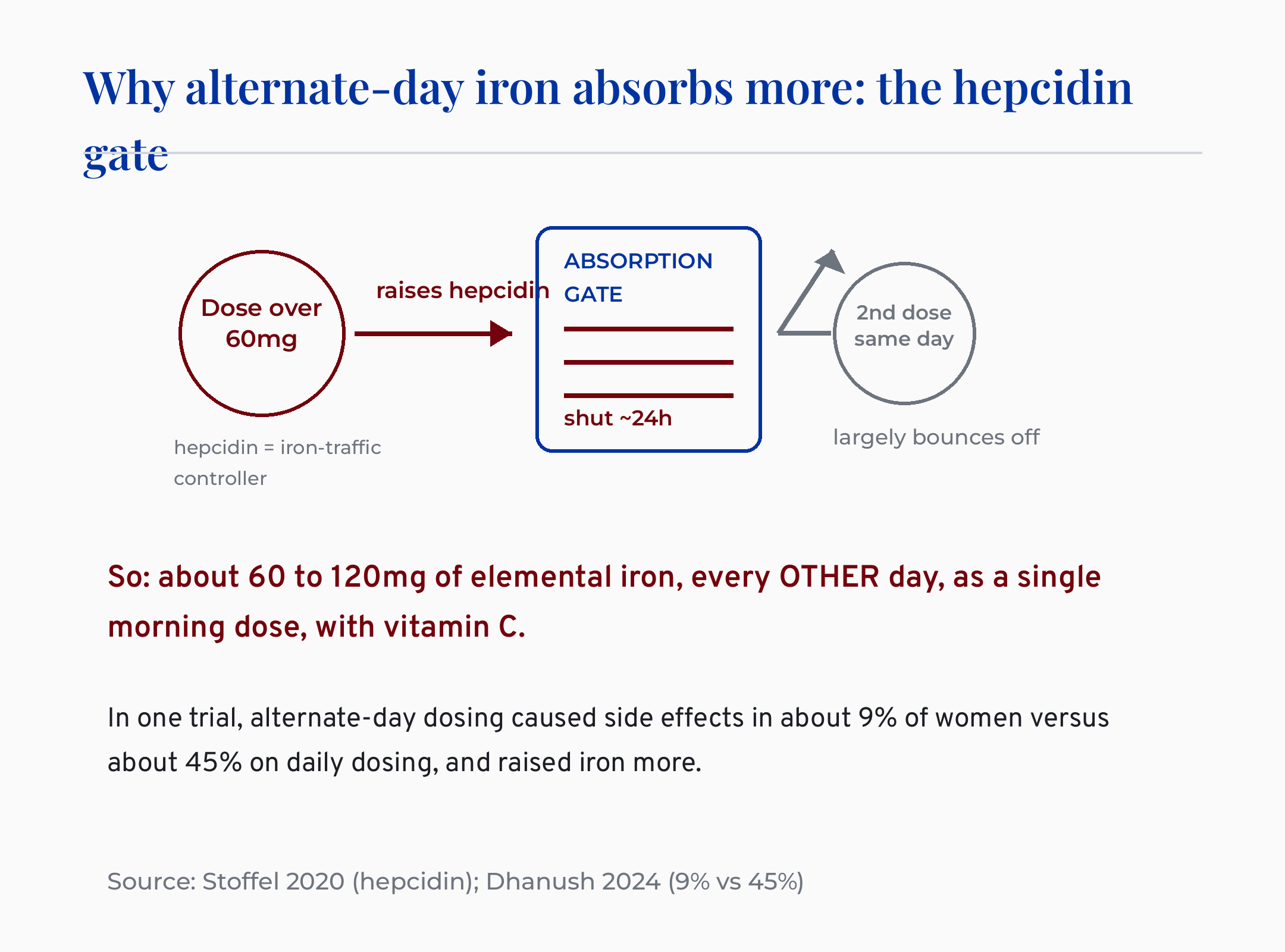
The reason is a hormone called hepcidin, meaning the body’s iron-traffic controller. When you take a large iron dose, hepcidin rises and slams the absorption door shut for about a day. So a second same-day dose largely bounces off.
One iron dose over 60mg raises hepcidin for 24 hours, so alternate-day morning dosing absorbs more. This is one of those rare moments where the modern research and the naturopathic instinct land in the same place. Alternate-day, single-morning, with vitamin C is both what the trials support and what thoughtful natural-medicine practice already leaned toward.
The tolerability payoff is real too. In a recent trial, alternate-day dosing caused adverse effects in about 9 percent of women, versus about 45 percent on daily dosing, and it actually raised iron levels more. Fewer gut symptoms and better absorption at the same time is an unusual win.
A few practical notes from how the research reads. Vitamin C alongside your iron boosts non-heme absorption. Keep iron away from coffee, tea, calcium, and especially thyroid medication, because they blunt absorption or get blunted in return.
If you have ever quit iron because it wrecked your stomach, this is your second chance. The problem may have been the schedule, not the iron.
What this means for you: about 60 to 120 mg of elemental iron, every other day, one morning dose, with vitamin C, away from coffee and your thyroid pill. After labs, never as a blind guess.
When is low iron a red flag, not just a supplement fix?
Some situations need a workup before any supplement, full stop. Blood in the stool, unexplained weight loss, or a deficiency that your periods cannot explain all point toward finding a source, not refilling a tank. These are not “take more iron” problems.
Iron is also not benign just because it is a nutrient. It is harmful in overload states like hemochromatosis, meaning a genetic condition where the body hoards too much iron. Loading high-dose iron into someone who is already overloaded does real damage.
And iron is dangerous in overdose, which is why it has to stay away from children. It is one of the leading causes of poisoning in young kids. A bottle of “just a vitamin” is not a casual thing in a house with toddlers.
If you are pregnant or breastfeeding, your iron dosing belongs to your prenatal provider, not to a blog. Your needs are different and the decisions are theirs to guide.
What this means for you: confirm deficiency with labs before you supplement, never megadose, and treat the red-flag symptoms as a reason to investigate rather than to self-treat.
How does this connect to the other “your labs are normal” stories?
If this pattern feels familiar, it is because iron is one of several places where a “normal” lab hides a real problem. The diagnostic miss is the thread, not the nutrient. The same logic shows up across thyroid, hormones, and inflammation.
I have written through this exact shape before in this pillar. If your fatigue sits alongside thyroid questions, PCOS and Hashimoto’s: The Antibody Test No One Ran walks through the antibody test that gets skipped the same way ferritin does. The frame is identical: a normal-looking panel that never asked the right question.
If your “normal” labs sit next to confusing perimenopause changes, PCOS Has a New Name (PMOS): What Actually Changes for You covers how a label and a lab can both be reinterpreted once you look closer. And if your exhaustion comes with histamine and dismissed symptoms, Why a Normal Mold Panel Doesn’t Mean You’re Fine is the same “your panel was normal, here is how to actually read it” story in a different system.
What this means for you: a normal result is not the same as a thorough one. Knowing which number was missing is the whole game.
Ferritin decision card titled normal blood count still exhausted, summarizing which iron labs to ask for and how to dose
What I’d do this week
Here is the bookmarkable version. Save this, screenshot it, or read it to your doctor.
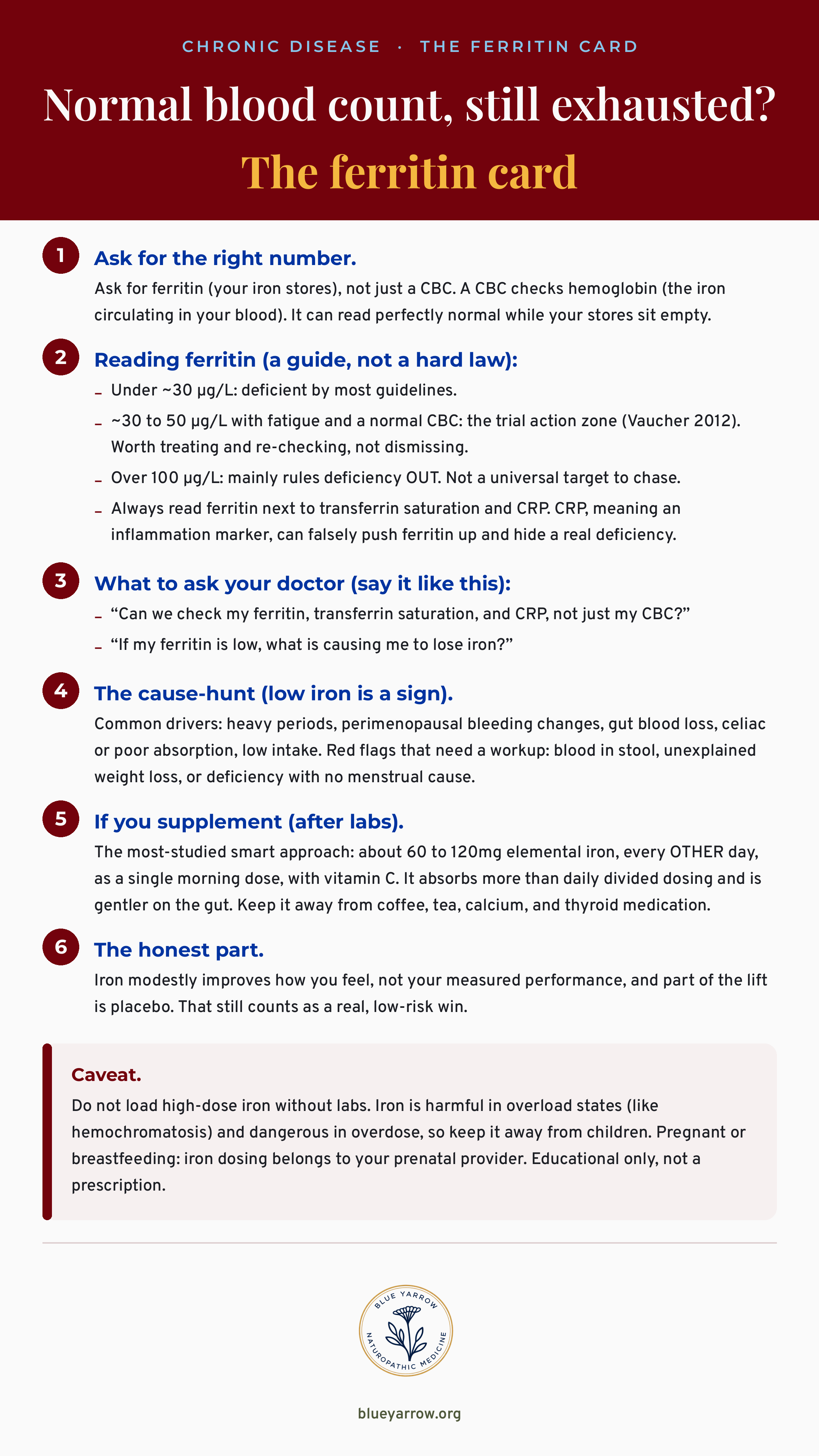
A note on how to read the evidence behind that card. The fatigue benefit has solid data behind it from two meta-analyses and a landmark trial. The “no performance gain” finding is equally solid. The alternate-day dosing has strong and growing support. The exact ferritin cutoff is the one piece that is genuinely still being argued, and I would rather tell you that than pretend it is settled.
The honest bottom line
You were not imagining the fatigue, and your doctor likely checked the wrong number. That is the validation, and it is true. Now here is the discipline that makes it useful.
Ferritin is the test that catches what a blood count misses. Below 50 with fatigue is worth acting on. Iron can genuinely help how you feel, though not how you perform, and some of that lift is placebo, which is honest, not disappointing. And low iron is a sign, so the real work is finding why you are losing it and dosing the smart way once you do.
So here is my one question for you this week. If you have felt dismissed with “normal” labs, will you go back and ask for ferritin, transferrin saturation, and CRP by name? I would love to hear what your number turns out to be.
Frequently asked questions
Can your iron be low if your blood count is normal? Yes. A complete blood count measures hemoglobin, the iron circulating in your blood, while ferritin measures your iron stores. Your body drains storage first to protect circulating blood, so ferritin can be low while a CBC reads perfectly normal. This is iron deficiency without anemia, and it is common.
What ferritin level is considered too low? Most guidelines call under about 30 micrograms per liter deficient. A ferritin between 30 and 50 with fatigue and a normal blood count is worth acting on and re-checking. The exact cutoff is still debated among specialties, ranging from 15 to 50, so context and symptoms matter alongside the number.
Does iron supplementation actually help fatigue? In non-anemic women with low ferritin, iron produces a modest but real reduction in self-reported fatigue. The honest caveat is that it does not improve measured physical performance, and a large share of the benefit also shows up on placebo. It is a real low-risk help, not a miracle fix.
What is the best way to take iron so it absorbs? Take iron every other day as a single morning dose with vitamin C. A large dose raises hepcidin, a hormone that blocks absorption for about a day, so alternate-day dosing absorbs more total iron and causes fewer gut side effects than daily dosing. Keep it away from coffee, calcium, and thyroid medication.
Should everyone aim for ferritin over 100? No. Ferritin over 100 mainly rules out deficiency and is a target in specific situations like restless legs or confirming full repletion. It is not an evidence-based universal optimum. Chasing 100 for everyone overstates what the research supports and is not the right goal for most women.
When is low iron a reason to see a doctor urgently? When iron is low without an obvious cause, or alongside blood in the stool, unexplained weight loss, or deficiency that your periods cannot explain. These warrant a workup to find a source of blood loss, not just a supplement. Low iron is a sign, so the cause matters more than the refill.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Houston, B. L., Hurrie, D., Graham, J., et al. (2018). Efficacy of iron supplementation on fatigue and physical capacity in non-anaemic iron-deficient adults: a systematic review of randomised controlled trials. BMJ Open, 8(4), e019240. https://doi.org/10.1136/bmjopen-2017-019240
2. Vaucher, P., Druais, P.-L., Waldvogel, S., & Favrat, B. (2012). Effect of iron supplementation on fatigue in nonanemic menstruating women with low ferritin: a randomized controlled trial. CMAJ, 184(11), 1247-1254. https://doi.org/10.1503/cmaj.110950
3. Yokoi, K., & Konomi, A. (2017). Iron deficiency without anaemia is a potential cause of fatigue: meta-analyses of randomised controlled trials and cross-sectional studies. British Journal of Nutrition, 117(10), 1422-1431. https://doi.org/10.1017/S0007114517001349
4. Stoffel, N. U., von Siebenthal, H. K., Moretti, D., & Zimmermann, M. B. (2020). Oral iron supplementation in iron-deficient women: How much and how often? Molecular Aspects of Medicine, 75, 100865. https://doi.org/10.1016/j.mam.2020.100865
5. Low, M. S. Y., Speedy, J., Styles, C. E., De-Regil, L. M., & Pasricha, S. R. (2016). Daily iron supplementation for improving anaemia, iron status and health in menstruating women. Cochrane Database of Systematic Reviews, 4, CD009747. https://doi.org/10.1002/14651858.CD009747.pub2
6. Dhanush, M., Vinod, K. V., Manivannan, P., et al. (2024). Daily versus alternate day oral iron replacement for women with iron deficiency anaemia: a randomized controlled trial. Indian Journal of Hematology and Blood Transfusion, 41(2), 245-251. https://doi.org/10.1007/s12288-024-01816-9