Perimenopause Migraine: It’s Estrogen, Not Histamine
Have you noticed your migraines used to arrive with your period, and now they show up whenever they want? That shift is real, and it has a name. Here is the plain answer most of the internet skips.
Women get migraine roughly 3 times more than men, and perimenopausal attacks track estrogen withdrawal, not histamine (Warfvinge 2026). I am Dr. Shad Abdulla, ND, and I want to give you the honest version of this, because the wellness world handed you a tidier story than the evidence supports. I will walk you through what is actually driving these headaches, where histamine genuinely fits, what helps first, and the red flags worth knowing.
This is Part 1 of 3 in my perimenopause migraine series.
Why do your perimenopause migraines feel like they came out of nowhere?
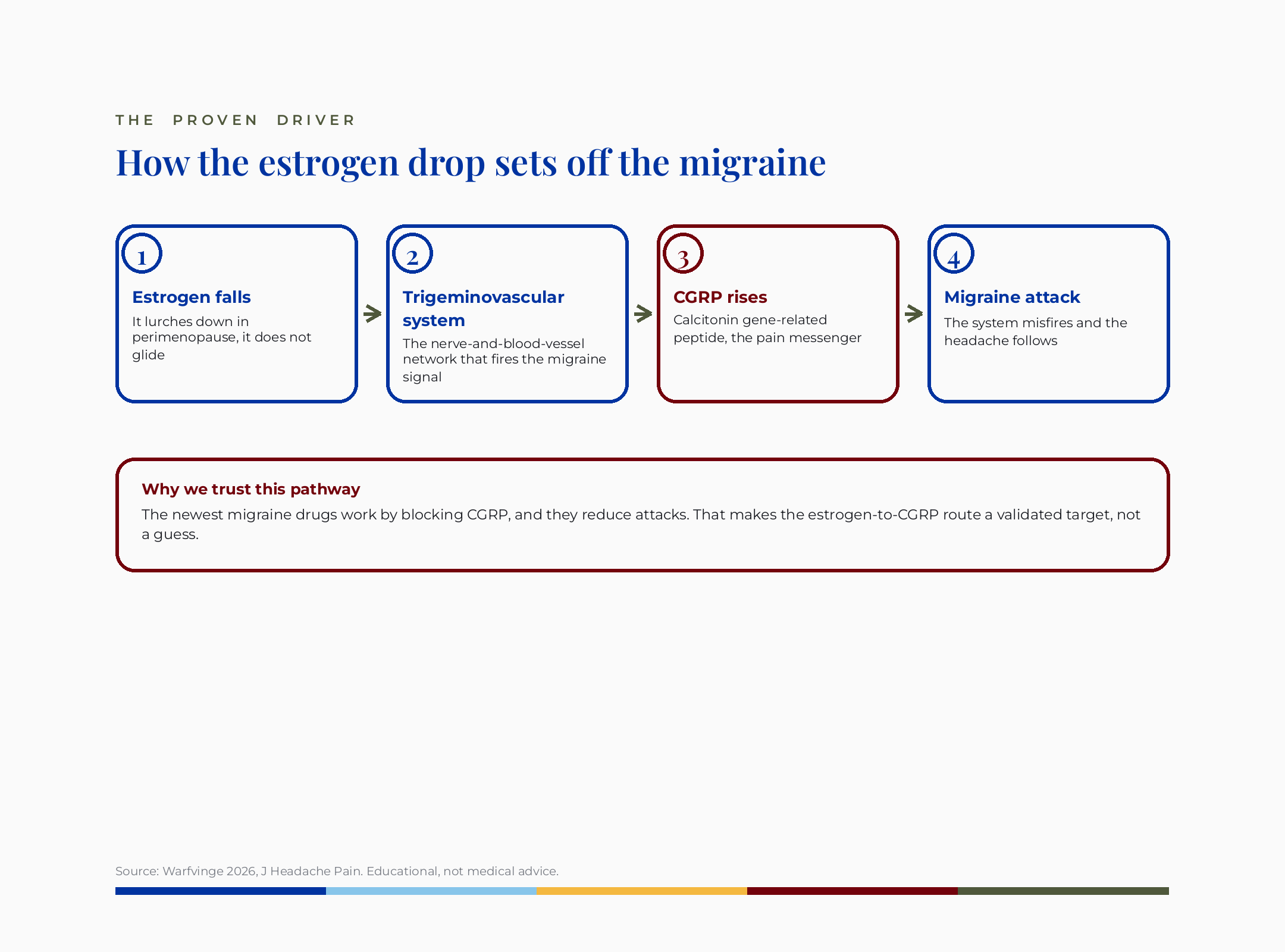
They feel sudden because your hormones stopped being predictable, not because your body forgot how to handle food. In perimenopause, estrogen does not glide down a ramp. It lurches. That lurching is what your nervous system reacts to.
Here is what conventional medicine misses when it just hands you a triptan and moves on. It treats the attack and skips the why. The naturopathic lens on this starts with the root cause, which is the hormonal drop itself, and then asks what stabilizes it.
Let me explain the mechanism in plain words. Migraine pain runs through the trigeminovascular system. That term means the nerve-and-blood-vessel network in your head that fires off the migraine pain signal. When estrogen falls, that system gets more sensitive and more likely to misfire.
The research goes one level deeper, and it is the part I find most convincing. Estrogen is closely tied to a pain messenger called CGRP, meaning calcitonin gene-related peptide, the chemical that the newest migraine drugs are built to block (Warfvinge 2026). When those CGRP drugs reduce attacks, that tells us the estrogen-to-CGRP pathway is not a guess. It is a validated target.
A woman I will call Renata, and her name is changed for privacy, described it exactly this way. Her migraines used to land like clockwork two days before her period. By her mid-forties they scattered across the whole month. Nothing about her diet had changed. Her cycle had.
The takeaway here: the suddenness you feel is the unpredictability of your estrogen, not a new food allergy. That single reframe changes what you do next.
Is your perimenopause migraine actually a histamine problem?
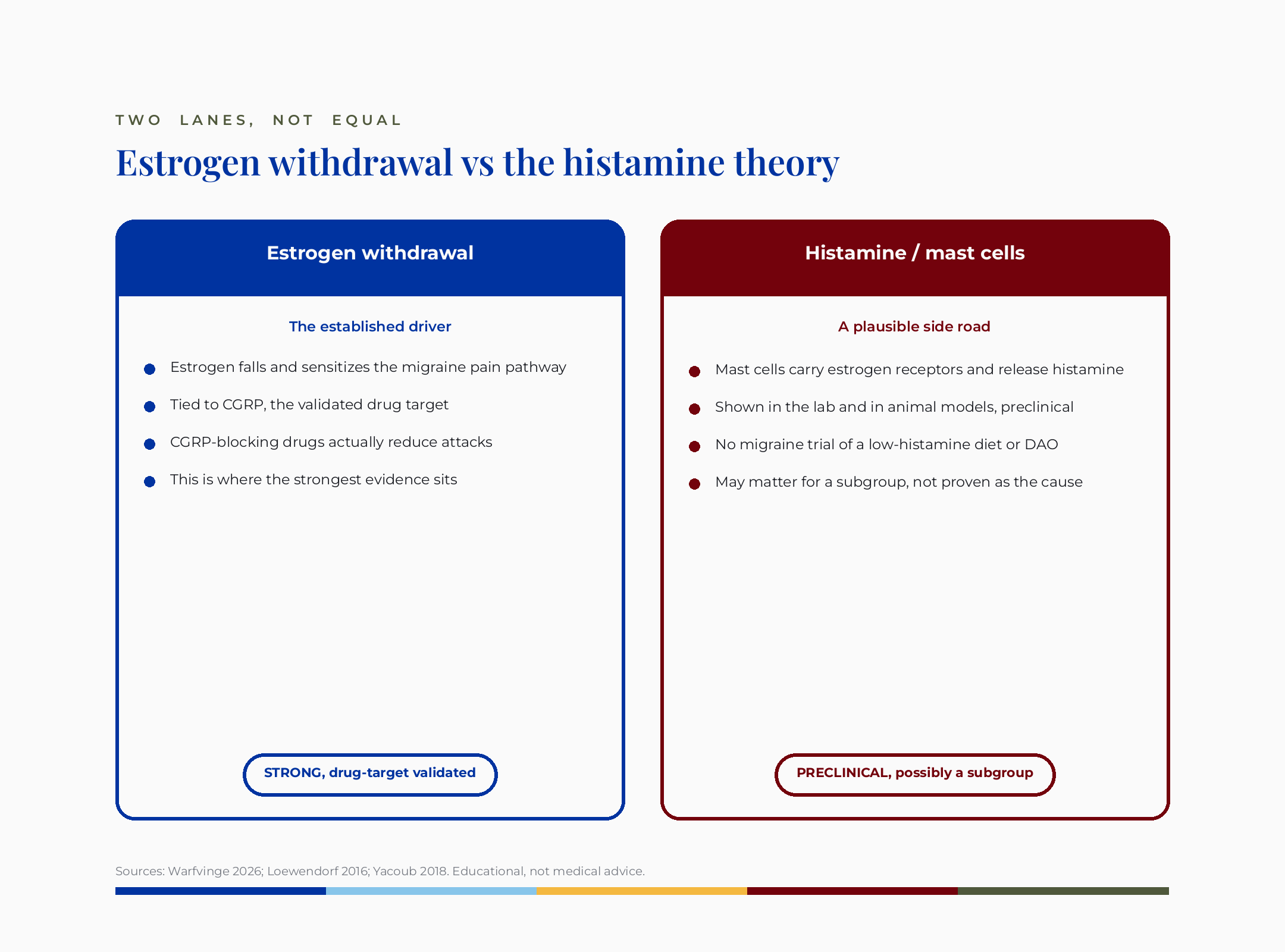
Probably not as the main driver, though histamine is not nothing. The honest answer is that estrogen withdrawal is the proven cause, and histamine is a plausible, mostly unproven, possibly-for-some-women contributor.
Here is where the wellness story comes from. Mast cells, meaning the immune cells that release histamine, carry estrogen and progesterone receptors, and they can release histamine and other chemicals that sensitize pain nerves. That is real biology (Loewendorf 2016). But it is preclinical, meaning it has been shown in the lab and in animal models, not proven to drive human migraine in a trial.
I want to be fair to both sides here, because the science deserves it. There is no migraine trial that tests a low-histamine diet. There is no migraine trial that tests DAO, meaning diamine oxidase, the enzyme that breaks down histamine in your gut. The closest study we have was done in hives.
The only DAO supplement trial was in hives, not migraine, and helped only the low-DAO subgroup (Yacoub 2018). That study had 22 women. It tested chronic hives, not headaches. And the benefit showed up only in the women who started with low DAO levels. That is a narrow signal, in the wrong condition, with a marker that is itself unreliable.
So when a creator tells you low estrogen broke your histamine clearance and that is why you get migraines, hold that loosely. It is a tidy single-cause story. The evidence does not support leading with it.
The takeaway here: histamine is a real but secondary and unproven player in migraine. Do not build your whole plan around a histamine diagnosis nobody can confirm.
Why does cutting wine sometimes help your headaches anyway?
Because cutting wine lowers your total trigger load, not because it proves a histamine defect. This is the both-and that almost no one says out loud, and it matters.
I hear this constantly from women who write to me. Wine and beer gave them the worst headaches, the stuffed sinuses, the next-day fog. Cutting it helped. That experience is real, and I would never tell you to ignore it.
Here is the honest mechanism. Alcohol is a known migraine trigger on its own. It dilates blood vessels, disrupts sleep, and adds to the pile of things your sensitized nervous system is already managing. Removing it helps because you removed a trigger, not because you fixed a broken enzyme.
In cases I have reviewed, the women who get the most relief are the ones who treat alcohol and aged foods as load reducers, not as cures. One woman I worked with, her name changed for privacy, cut wine and felt better, then assumed she had to eliminate forty foods. The forty-food version made her anxious and undernourished and did not help more.
That is the cost worth naming. A long-term restrictive low-histamine diet carries real risks: nutritional gaps, disordered-eating patterns, and false reassurance that delays better-supported care. Cutting one or two clear triggers is smart. Eliminating half your plate is not.
The takeaway here: removing wine and obvious triggers is a reasonable, free first move. Just call it what it is, which is lowering your total load.
What actually helps perimenopause migraine first, without buying anything?
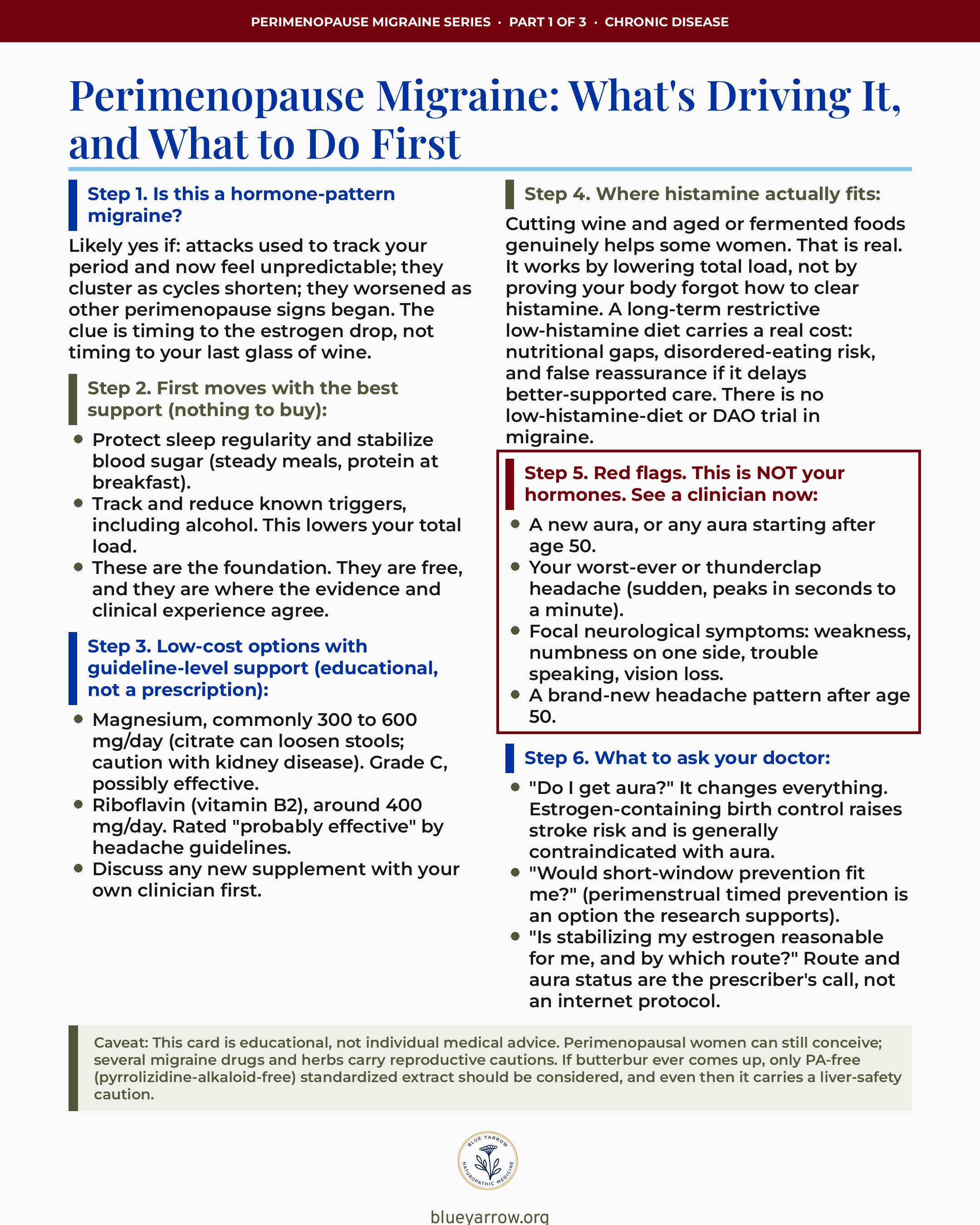
The two highest-value moves cost nothing: protect your sleep regularity and steady your blood sugar. This is where the evidence and clinical experience actually agree, and it is the least glamorous part, which is why the internet skips it.
Sleep matters because irregular sleep is one of the most reliable migraine triggers we have. Going to bed and waking at consistent times, even on weekends, takes pressure off the same sensitized system estrogen is already stressing. Steady meals with protein at breakfast keep your blood sugar from swinging, and blood-sugar swings are their own trigger.
This is the foundation in my naturopathic training, and it is the root-cause version of the question. Before any supplement, before any prescription, you stabilize the inputs that feed the attack. In cases I have reviewed, women who fix sleep and meals first often need less of everything else.
Track your triggers too, including alcohol. A simple log of what preceded each attack tells you more than any expensive test. You are looking for your own pattern, not someone else’s.
The takeaway here: sleep regularity, protein at breakfast, and a trigger log are free, evidence-aligned, and the first thing I would do. Start there before you spend a dollar.
Do magnesium and riboflavin really help migraine?
Yes, both have guideline-level support as low-cost prevention options, which puts them in a different class than DAO. This is the part where conventional and naturopathic care actually shake hands.
Magnesium earns Grade C, possibly effective for migraine prevention near 600 mg daily, guideline-backed and low-cost (von Luckner 2017). Grade C means possibly effective, which is honest, not weak. It shows up in mainstream neurology guidelines, and it is cheap. The common range is 300 to 600 mg a day.
A practical note on form. Magnesium citrate can loosen your stools, so some women do better splitting the dose or choosing a gentler form. If you have kidney disease, magnesium needs a clinician’s oversight, full stop.
Riboflavin, meaning vitamin B2, is rated probably effective by headache guidelines, usually around 400 mg a day. It is well tolerated and inexpensive. Both of these are what I mean when I say there are better-supported levers than a histamine stack.
I want to name the uncertainty cleanly, because that honesty is the whole point. These are possibly-to-probably effective, not guaranteed. They help some women meaningfully and others not at all. That is still a better bet than a supplement with no migraine trial behind it.
The takeaway here: magnesium near 300 to 600 mg and riboflavin near 400 mg are guideline-supported, cheap, and worth a conversation with your clinician. Ask about them by name.
Can stabilizing your estrogen help, and is it safe?
It can help reduce attack frequency, but it is genuinely more nuanced than the internet says, and it is a prescriber’s decision, not an internet protocol. Two things have to travel together here: the potential benefit and one hard safety line.
Smoothing out the estrogen drop can reduce migraine frequency for some women, because you are softening the exact lurch that sets off attacks. The route matters, the dose matters, and your individual risk matters. This is not a supplement you self-select. It is a medical conversation.
Now the safety line, and please read this part twice. If you have migraine with aura, meaning visual or sensory changes like flashing lights or tingling before an attack, estrogen-containing birth control raises your stroke risk and is generally contraindicated (Cappy 2015). Aura plus estrogen-containing contraception is a documented red line. This is why your aura status changes everything.
Menopausal hormone therapy is a different risk profile from contraceptive-dose estrogen, and transdermal routes are generally considered lower-risk than oral. But I am not going to hand you a route or a dose from a blog. That is exactly the call your prescriber makes after assessing your aura status and your full history.
What the research supports, and what I would want you walking in knowing, is that short-window prevention timed to your cycle is a real option (Khoo 2024). About a quarter of women with migraine have menstrual migraine, the kind tied to your cycle, and it tends to be more severe and harder to treat. There are timed approaches the evidence backs.
The takeaway here: stabilizing estrogen can help, but aura status and route make it a prescriber decision. Walk in knowing your aura status, because it changes what is safe for you.
When is a perimenopause headache a red flag, not your hormones?
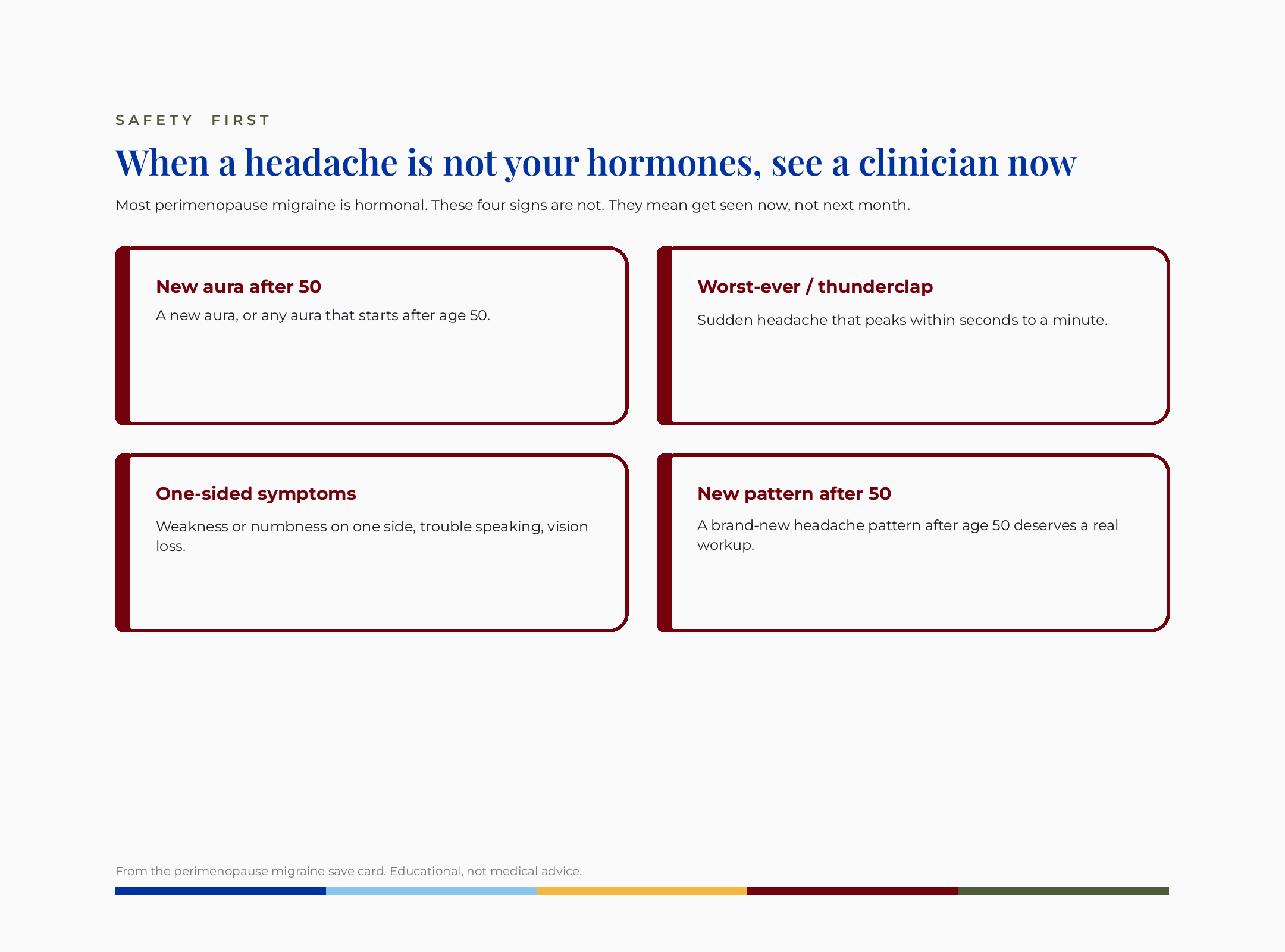
Some headaches are not hormonal and need a clinician now, not next month. Safety is authority, so I will be direct. Most perimenopause migraine is your hormones. These specific signs are not, and they deserve urgent attention.
See a clinician promptly for a new aura, or any aura that starts after age 50. See someone for your worst-ever or thunderclap headache, meaning one that peaks within seconds to a minute. Get help for focal neurological symptoms: one-sided weakness or numbness, trouble speaking, or vision loss. And a brand-new headache pattern after age 50 deserves a real workup.
I am not saying this to frighten you. I am saying it because the kind doctor tells you the honest version, including the part where some headaches are signals you should not sit on. Knowing these lines is part of advocating for yourself.
The takeaway here: new aura after 50, worst-ever or thunderclap headache, and one-sided neurological symptoms are red flags. They mean see someone now, not later.
What I’d do this week
Here is the decision card I would want a friend to save. Mechanism and timing only, no brands. This is educational, not a prescription, so bring it to your own clinician.
If you want the companion piece on the antihistamine question, I wrote one. The viral Pepcid and Claritin for perimenopause approach is not proven for migraine, and that post explains why. And if your reactions feel bigger than your cycle alone, my piece on Mold-driven histamine load covers the environmental angle.
The honest bottom line
Your perimenopause migraines are mostly an estrogen-withdrawal problem, not a histamine problem, and that distinction changes what actually helps. The food reactions are real. The suddenness is real. But the migraine itself is driven by estrogen falling and fluctuating, and the best first moves follow from that.
I built Blue Yarrow because I want to share my naturopathic doctor training and knowledge so that people who are not getting answers from conventional doctors can find the answers with me. If you have read this far, thank you. Which part of your migraine pattern finally makes more sense now, the timing or the triggers?
Frequently asked questions
Is perimenopause migraine caused by histamine intolerance? Most likely no, at least not as the main driver. The proven cause is estrogen withdrawal acting on the migraine pain pathway. Histamine and mast cells are a plausible but mostly preclinical contributor, with no migraine-specific trial behind them. Cutting high-histamine foods may help some women by lowering total trigger load.
Does a low-histamine diet help migraines? There is no migraine trial testing a low-histamine diet, so we cannot say it treats migraine. Some women feel better cutting wine and aged foods, which likely reduces overall triggers rather than fixing a histamine problem. A strict long-term version carries real risks, including nutritional gaps and disordered eating.
What is the best natural supplement for perimenopause migraine? Magnesium and riboflavin have the strongest guideline support among low-cost options. Magnesium near 300 to 600 mg daily is rated possibly effective, and riboflavin near 400 mg daily is rated probably effective. Discuss doses with your clinician, especially magnesium if you have kidney disease.
Can hormones stop my perimenopause migraines? Stabilizing estrogen can reduce attack frequency for some women, but route, dose, and your aura status all matter, so it is a prescriber decision. If you have migraine with aura, estrogen-containing birth control raises stroke risk and is generally contraindicated. Always have your aura status assessed first.
When should I worry about a perimenopause headache? See a clinician promptly for a new aura or any aura starting after age 50, your worst-ever or thunderclap headache, one-sided weakness, numbness, trouble speaking, or vision loss, or a brand-new headache pattern after 50. These are red flags that are not your hormones and need urgent attention.
Why do migraines get worse in perimenopause? Because estrogen stops falling smoothly and starts lurching, and that unpredictable drop sensitizes the migraine pain pathway. Menstrual migraine, the kind tied to your cycle, tends to get harder to treat in this window. About a quarter of women with migraine have this subtype, and it is more severe and longer-lasting.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Reference
1. Warfvinge, K., Edvinsson, J. C. A., Maddahi, A., & Edvinsson, L. (2026). Hypothalamic and sex-related hormones in migraine. The Journal of Headache and Pain, 27(1). https://doi.org/10.1186/s10194-026-02289-z
2. Khoo, C. C., Liu, C. C., Lu, M., Huang, Y. C., & Weng, H. Y. (2024). Acute and preventive treatment of menstrual migraine: A meta-analysis. The Journal of Headache and Pain, 25(1), 143. https://doi.org/10.1186/s10194-024-01848-6
3. von Luckner, A., & Riederer, F. (2017). Magnesium in migraine prophylaxis: Is there an evidence-based rationale? A systematic review. Headache, 58(2), 199-209. https://doi.org/10.1111/head.13217
4. Cappy, H., Lucas, C., Catteau-Jonard, S., & Robin, G. (2015). Migraine and contraception. Gynecologie Obstetrique & Fertilite, 43(3), 234-241. https://doi.org/10.1016/j.gyobfe.2015.01.006
5. Loewendorf, A. I., Matynia, A., Saribekyan, H., Gross, N., Csete, M., & Harrington, M. (2016). Roads less traveled: Sexual dimorphism and mast cell contributions to migraine pathology. Frontiers in Immunology, 7, 140. https://doi.org/10.3389/fimmu.2016.00140
6. Yacoub, M. R., Ramirez, G. A., Berti, A., Mercurio, G., Breda, D., Saporiti, N., Burastero, S., Dagna, L., & Colombo, G. (2018). Diamine oxidase supplementation in chronic spontaneous urticaria: A randomized, double-blind placebo-controlled study. International Archives of Allergy and Immunology, 176(3-4), 268-271. https://doi.org/10.1159/000488142
7. Waliszewska-Prosol, M., Grandi, G., Ornello, R., Raffaelli, B., Straburzynski, M., Tana, C., & Martelletti, P. (2025). Menopause, perimenopause, and migraine: Understanding the intersections and implications for treatment. Neurology and Therapy, 14(3), 665-680. https://doi.org/10.1007/s40120-025-00720-2