Normal Labs, Still Shedding: What “Normal” Misses
Here is what conventional medicine usually misses with hair thinning in women. It looks at your thyroid number, your blood count, maybe your iron, sees results inside the reference range, and tells you everything is fine. The honest answer is that a hair-loss workup with in-range labs is rarely finished, it is just paused. Most women shedding do not have an androgen excess, an in-range lab is not the same as an optimal one, and no study has ever shown that nudging a normal number regrows hair. So this is the root-cause version of the question: find and fix a true deficiency, and stop chasing a number on a chart. I read the actual studies for a living, and I want to walk you through what the evidence really supports, not what the supplement aisle sells. None of this replaces your own clinician. It is here to make you harder to dismiss.
“My blood work came back normal, so why am I still losing hair?”
Because normal is a population range, not your personal optimum, and because the thing driving your shedding may not be a single lab at all. A reference range is built from a large group of people. It tells you whether you are an outlier, not whether you are thriving.
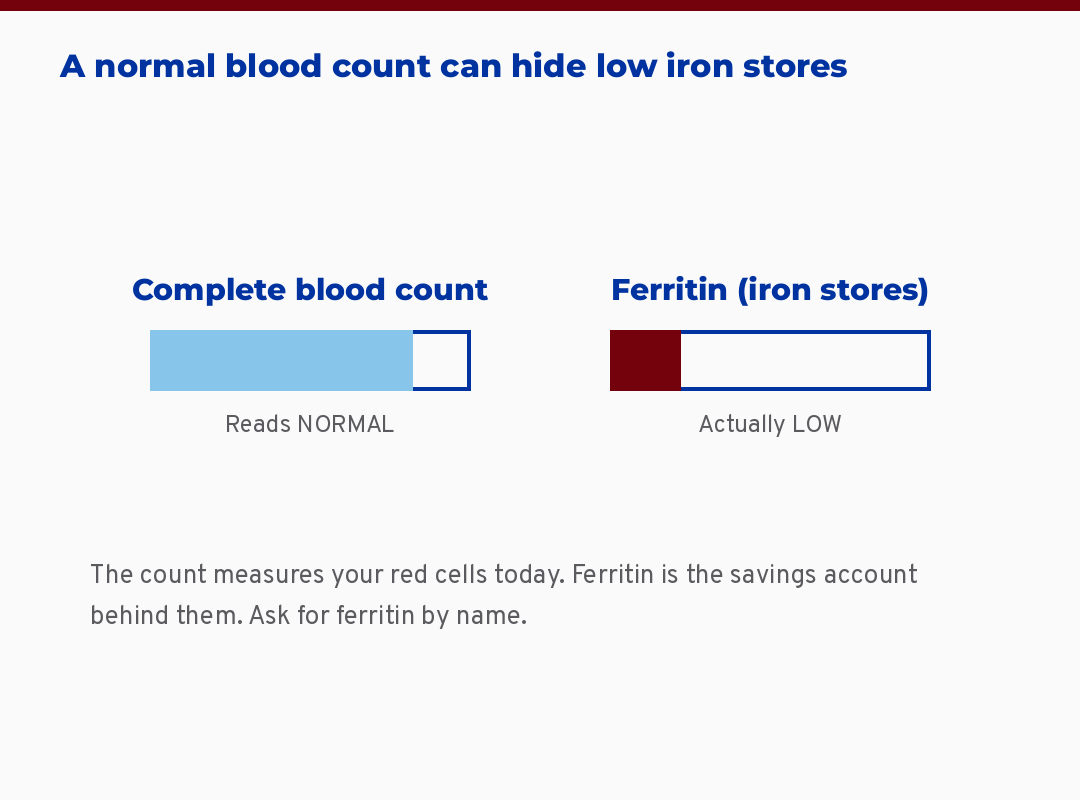
Two gauges showing a normal complete blood count beside a low ferritin reading
Here is the thing. The most common pattern I see described, again and again, is a woman whose ferritin, meaning the protein that stores your iron, lands somewhere in the middle of the range, whose thyroid-stimulating hormone (TSH, the pituitary signal that tells your thyroid how hard to work) reads normal, and who is still finding hair on her pillow, in the shower drain, wrapped around her fingers. She is told it is stress, or age, or genetics. Sometimes that is true. Often the workup simply stopped too early.
What this means for the woman reading this: a normal result is not a closed door. It is a reason to ask better questions about which test was run, what the number actually was, and what was never checked at all.
The short version: a lab inside the normal range is not the same as optimal, and a single normal TSH does not rule out a thyroid problem.
Is it the iron, the thyroid, the hormones, or the stress?
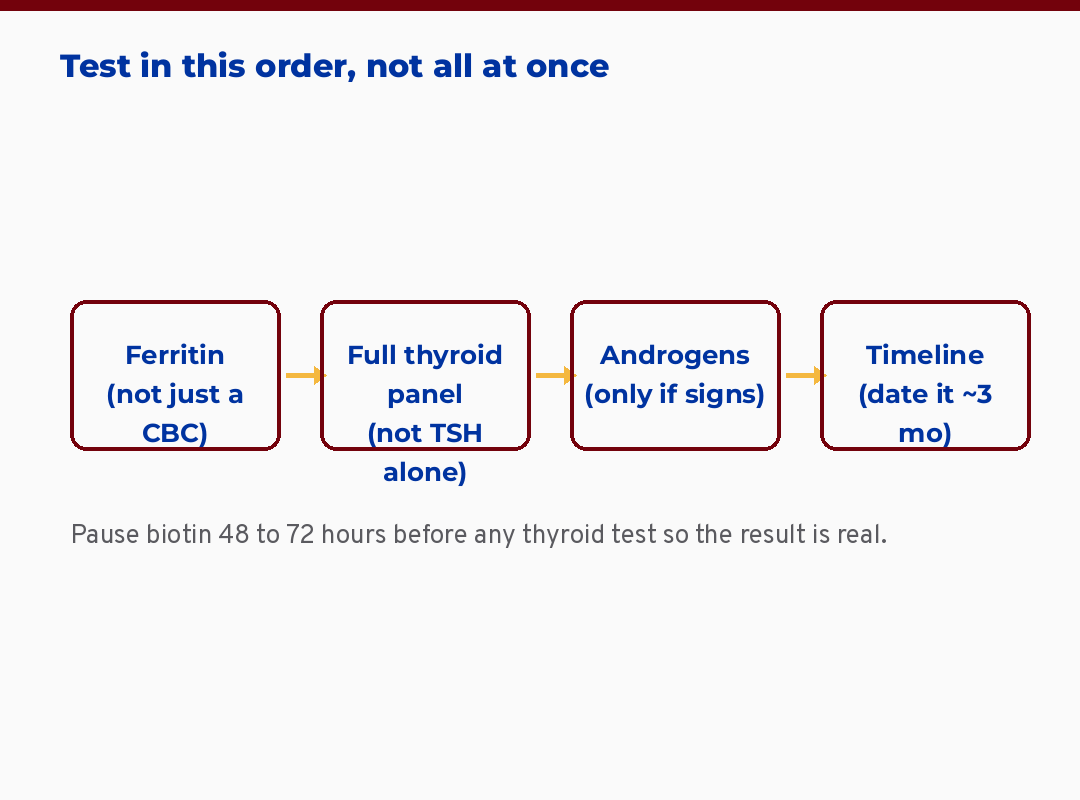
It is usually one or two of those, and the way to stop drowning in causes is to test in an order instead of all at once. The overwhelm is real. Every reel gives you the same five-test list and no sequence. Let me give you the reasoning instead.
Iron is the first stop for most women, especially if you have heavy periods. The association is genuine. Women with hair shedding average 18.5 ng/dL lower ferritin than unaffected women (Treister-Goltzman 2021, n=10,029). That is a large, pooled analysis, and it is real. But notice the word association. It tells us shedding women tend to have lower stores. It does not prove that raising the number grows the hair back.
Thyroid is the second stop. The thyroid axis directly regulates the growth phase of the follicle, which is why diffuse thinning can be the first visible sign that something is off. The catch is the test. A lone TSH can read normal while early thyroid autoimmunity is already underway.
Hormones are the third stop, and here is the part most women are never told. Only about one-third of women with female pattern hair loss have abnormal androgens (Starace 2020). So the default story, that thinning means too much testosterone, is wrong most of the time.
Stress is the fourth, often through a pattern called telogen effluvium, which I will explain in plain terms below.
What this means for you: you do not need every test at once. You need the right test, in the right order, read against the right number.
What is telogen effluvium, and will my hair grow back?
Telogen effluvium is a shift in the hair cycle where more follicles than usual drop into their resting-and-shedding phase at the same time, and in most cases it recovers. Think of your scalp as a field where each plant is on its own clock. Normally they cycle out of sync, so the field always looks full. A big stressor, an illness, a pregnancy, a crash diet, a hard season, can push a whole cohort into the resting phase together. About three months later, they shed together. That is the scary handful in the shower.
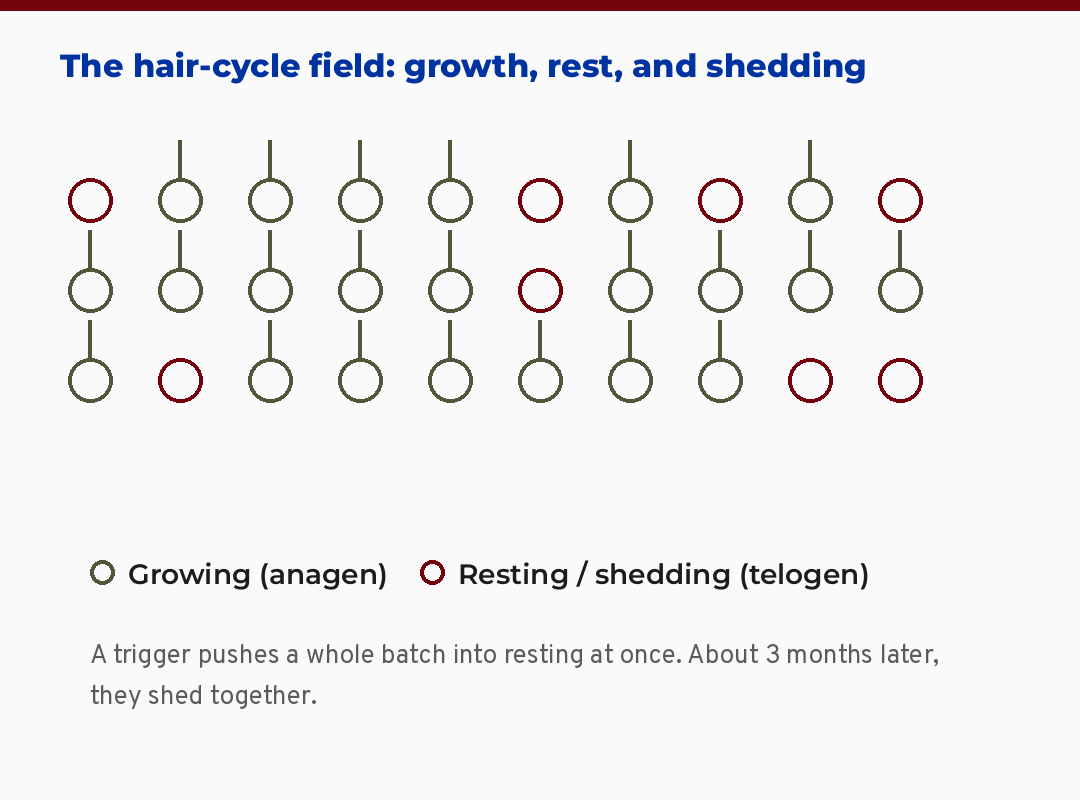
Diagram of the hair-cycle field showing most follicles growing while some rest and shed together
The good news is the part that gets buried. This kind of shedding is a cycle shift, not permanent follicle loss, and it commonly recovers once the trigger passes. The skill is dating it. In cases I have reviewed, the single most useful question is what was happening about three months before the shedding started. Name the trigger and the timeline stops feeling like a free fall.
This is different from the gradual thinning at the part line and the temples that signals female pattern hair loss, where follicles slowly shrink. The two can overlap, which is exactly why a careful history matters more than another panel.
The short version: shedding that started after a clear trigger about three months earlier usually recovers. Gradual thinning at the part is a different conversation.
Should I get my ferritin over 70 to regrow my hair?
No, not as a guarantee, because the popular “ferritin over 70” rule is a clinical-consensus target, not a proven regrowth threshold. This is where I part ways with a lot of the root-cause content you have seen, and I want to be honest about why.
The number gets repeated as if it were settled. It is not. Above a ferritin of 10, iron stores show no link to hair loss activity in women (Bregy and Trueb 2008). A large US study found no increase in iron deficiency in female pattern hair loss or chronic shedding compared to women without hair loss, and at the lowest cutoff, deficiency was actually more common in the comparison group than in the women losing hair (Olsen 2010). No trial has tested raising ferritin to any specific target and measured real regrowth in women whose labs are already in range.
Here is the naturopathic lens on this, and it is the part I care about most. Holding two true things at once is the honest position. A real, confirmed iron deficiency is worth finding and correcting, and it is low-risk to do so, especially with heavy periods. And a number on a lab sheet is not a promise that your hair comes back. The wellness world sells you the second claim to get you to the supplement. I would rather you keep your money and your trust.
What this means for the woman in front of me: if your iron is genuinely depleted, repletion is reasonable. If you are chasing 70 because an influencer said so, you are likely chasing a number, not a cause. For the fuller picture on why low stores cause symptoms long before classic anemia shows up, this companion read on iron deficiency without anemia and the fatigue it drives goes deeper than I can here.
What about vitamin D and zinc?
Two more nutrients are worth checking, with the same rule as iron: correct a real deficiency, do not chase a number. Vitamin D is the one that actually turns up low a lot. In a study of more than 3,000 people with this kind of shedding, nearly three-quarters were vitamin D deficient (Yorulmaz 2021), and in a female pattern hair loss group only about a third had a normal level (Siah 2016). No trial proves that topping it up regrows hair, but a true deficiency is common, easy to check, and low-risk to correct, so it earns a place on the list.
Zinc is the opposite story, and this one saves you money. It is in nearly every hair supplement, but actual zinc deficiency is uncommon in women who shed, only about 2% in that large group (Yorulmaz 2021). Repletion seems to help only people who are genuinely low, and taking it when you are not can backfire by depleting copper. So check it if there is a real reason to, and skip the blanket zinc gummy if your level is fine.
The short version: vitamin D is commonly low and worth correcting if it is, while zinc is rarely the problem, so test before you supplement.
If I still have my period, can it really be hormonal?
Yes, it can, because the hormonal environment of the follicle starts shifting in perimenopause years before periods become irregular. This is one of the most common misconceptions stated as fact: regular cycles, therefore not hormonal. The follicle does not work that way.
Estrogen acts directly on the hair follicle, which is an estrogen-sensitive tissue. As estrogen begins its long, bumpy decline through the early-to-mid forties, the follicle environment changes even while you are still bleeding monthly. That is part of why new thinning can begin around 41 to 45 with a perfectly normal cycle. You are not too young for this, and you are not imagining it.
I want to name something I see braided into these stories: the grief. Hair is identity, and being told you are fine while you watch your part widen is its own particular loneliness. The biology is real. So is the feeling. If the perimenopause angle resonates, the way estrogen’s decline ripples through more than your follicles is worth understanding, and this piece on the estrogen shift through perimenopause maps that terrain.
The short version: regular periods do not rule out a hormonal contribution. The follicle feels the estrogen shift before your cycle does.
What is the right way to check my thyroid for hair loss?
Ask for a full panel, not TSH alone, because a single normal TSH can sit on top of early thyroid autoimmunity that the one-test screen misses. The root-cause version of a thyroid workup includes TSH, free T4, free T3, and the antibodies, anti-TPO and anti-Tg.
The reason is mechanism. Thyroid autoimmunity, where the immune system slowly targets the thyroid, often shows up as positive antibodies long before TSH drifts out of range. A woman can have a textbook-normal TSH, positive anti-TPO, real symptoms, and a doctor who says everything is fine because the one number checked was fine. For how the thyroid picture overlaps with other patterns and why the panel matters, I walk through the full thyroid panel reasoning here.
One practical, genuine safety point. High-dose biotin, the B vitamin in nearly every hair-and-nails supplement, distorts lab assays. It can fake a thyroid panel and even skew a cardiac troponin test, which has sent people down the wrong path. This is not about whether biotin grows hair. It is about not corrupting the very test you are about to run. Stop biotin 48 to 72 hours before any blood draw.
What this means for you: if you are going to test your thyroid, test it properly, and pause the biotin first so the result is real.
Do the “natural” hair treatments actually work?
Some have a real mechanism and even a real trial behind them, but most of the strongest evidence was gathered in men or without a placebo group. So the honest answer is that the science here is more interesting, and more uneven, than either the marketing or the dismissals admit. I say this as someone with deep respect for botanical medicine, which is exactly why I want to tier it honestly instead of overstating it or waving it away.
Start with the one everyone shares. Rosemary is not just folklore, it has a real mechanism. Rosemary leaf extract blocks 5-alpha-reductase, the enzyme that converts testosterone into DHT, meaning dihydrotestosterone, the androgen that shrinks follicles. That is the same pathway the prescription drug finasteride works on. In the lab, rosemary inhibited that enzyme by over 80%, and its active compound kept DHT from binding the follicle’s receptor (Murata 2013). That is a genuine antiandrogen mechanism, not a vibe. The honest catch is the human evidence: the trial people cite, where rosemary oil matched 2% minoxidil, was done in men (Panahi 2015). So rosemary is mechanistically plausible and reasonable to try as a low-risk topical, while no female trial has confirmed it yet.
A few others sit in that same honest bucket. Caffeine, applied topically, also blocks 5-alpha-reductase and nudges the follicle (Herman 2013), with small trials but no definitive female data. Saw palmetto works on the same DHT pathway, borrowed from prostate research, promising in theory and unproven for women’s hair. Pumpkin seed oil has a positive trial, but it was male-only and a multi-ingredient blend.
Then the one almost nobody mentions, which actually has the strongest data in women. Sandalore, a synthetic sandalwood scent, is the surprise. Your hair follicles carry an olfactory receptor called OR2AT4, and stimulating it signals the follicle to stay in its growth phase longer (Chéret 2018). In a randomized, double-blind, placebo-controlled trial of 60 women with shedding, a 1% topical version reduced hair loss and increased hair volume and the share of growing follicles over 24 weeks (Jimenez 2020). That is a real women-specific trial, which is rare in this space, and it is worth knowing precisely because it is not the one being marketed to you.
A word on the supplement most heavily advertised to women. Marine protein supplements, the Viviscal type, do have two placebo-controlled trials in women showing less shedding and more hair (Ablon 2015; Rizer 2015). I am giving you that honestly. I am also giving you the part the ads leave out: both trials were funded by the maker, which does not erase the result but does mean you hold it a little more loosely.
For comparison, topical minoxidil adds about 9 hairs per square centimeter over placebo, and still fails roughly 40% of women (2016 trial). That is the single best-evidenced regrowth option there is, and it still does not work for everyone. So when something is sold as working “as well as minoxidil,” ask which study, in whom, against what.
The field is moving fast, too, and I would rather you hear the names from me than from an ad. Copper peptides, the cosmetic ingredient aminexil, and a genuinely new investigational drug called PP405 that aims to switch dormant follicle stem cells back on are all at various stages of testing. I am watching them. None is ready to be sold to you as proven, and I will cover them properly as the evidence matures.
The short version: rosemary and caffeine carry a real DHT-blocking mechanism, Sandalore has the rare women’s trial, marine-protein supplements rest on industry-funded trials, and minoxidil, the strongest option, still helps only some. Honest curiosity, tiered evidence, no confident promises.
The gentle traditional layer, named honestly
The naturopathic tradition I trained in has always had a hair toolkit too: silicon-rich foods like nettle, horsetail, and oats, scalp massage to bring blood flow to the follicle, and a steady, anti-inflammatory plate. I have a real fondness for these. I will also be straight with you about their tier. They are tradition and gentle self-care, with little or no trial evidence for regrowth, so I offer them as low-risk support that pairs well with finding the real driver, never as the fix on their own.
What I’d do this week
If you take one thing from this, take the list below. It is the order I would think in, and the questions I would walk in with. Screenshot it.

The expectation I would set: even when you find and fix the right thing, the follicle works on its own clock. Regrowth runs on a three-to-six-month horizon, not a three-week one. Patience here is not passivity. It is biology.
A realistic close
You came in through a vanity door and I have walked you toward a whole-person one, because that is where the answers actually live. The patterns I have described, low iron stores, quiet thyroid autoimmunity, the perimenopause shift, the stress-driven cycle shift, are the upstream signals this kind of thinning points to. Most of them are checkable. None of them respond to a number you simply will into range.
If you have been dismissed with a normal lab, you are not crazy and you are not vain. You are reading the situation more accurately than the five-minute appointment allowed. Take the list. Ask the better questions. Be a little harder to wave off.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Frequently asked questions
My blood work came back normal. Now what? Normal means you are inside a population range, not that the workup is finished. Check which tests were actually run, the exact ferritin value, and whether a full thyroid panel with antibodies was done. A normal complete blood count can sit alongside depleted iron stores or early thyroid autoimmunity that a single screening test misses.
Will my hair grow back? It depends on the type. Shedding that followed a clear trigger about three months earlier, called telogen effluvium, commonly recovers once the trigger resolves. Gradual thinning at the part line, where follicles shrink over time, behaves differently. Either way, regrowth runs on a three-to-six-month horizon, so progress is slow before it is visible.
Does ferritin really need to be over 70? Not as a proven rule. Above a ferritin of 10, iron stores show no link to hair loss activity in women in the published data, and no trial has shown that reaching a specific target regrows hair. Correcting a true, confirmed deficiency is reasonable. Chasing a specific number because it is popular is not the same thing.
If I still have regular periods, can hair loss be hormonal? Yes. The hair follicle is estrogen-sensitive, and the estrogen environment begins shifting in perimenopause years before cycles become irregular. New thinning in the early-to-mid forties with a normal period is common and real, not imagined.
Do natural treatments like rosemary or saw palmetto work? They are promising but not established for women. Rosemary has a real mechanism, it blocks the 5-alpha-reductase enzyme that makes DHT, the same pathway as finasteride (Murata 2013), but the human trial that matched minoxidil was in men. Caffeine and saw palmetto work on that same pathway with thin female data. The one with the best women-specific evidence is the least marketed: Sandalore, a sandalwood-scent compound that reduced shedding in a randomized trial in women (Jimenez 2020). Marine-protein supplements have women’s trials too, though both were funded by the maker. Worth honest curiosity, tiered by the evidence, not confident promises.
Should I take vitamin D or zinc for hair loss? Check them, do not blindly supplement. Vitamin D is commonly low in women who shed, so correcting a true deficiency is reasonable and low-risk, though no number guarantees regrowth. Zinc deficiency is actually uncommon here, so test before you supplement, and pair it with copper if you do.
Should I stop taking biotin? Not necessarily, but pause it before lab testing. High-dose biotin distorts lab assays and can fake a thyroid panel and other tests. Stop it 48 to 72 hours before any blood draw so your results are accurate.
References
1. Treister-Goltzman Y, Yarza S, Peleg R. Iron deficiency and nonscarring alopecia in women: systematic review and meta-analysis. Skin Appendage Disord. 2021. https://doi.org/10.1159/000519952
2. Olsen EA, Reed KB, Cacchio PB, Caudill L. Iron deficiency in female pattern hair loss, chronic telogen effluvium, and control groups. J Am Acad Dermatol. 2010. https://doi.org/10.1016/j.jaad.2009.12.006
3. Bregy A, Trueb RM. No association between serum ferritin levels >10 ug/l and hair loss activity in women. Dermatology. 2008. https://doi.org/10.1159/000118505
4. Starace M, Orlando G, Alessandrini A, Piraccini BM. Female androgenetic alopecia: an update. Am J Clin Dermatol. 2020. https://doi.org/10.1007/s40257-019-00479-x
5. Phase III randomized controlled trial of 5% minoxidil foam versus vehicle in women with FPHL. J Drugs Dermatol. 2016. PMID 27391639
6. Gaspar E, et al. Thyrotropin-releasing hormone: a new player in human hair-growth control. FASEB J. 2009. https://doi.org/10.1096/fj.08-126417
7. Ohnemus U, et al. The hair follicle as an estrogen target and source. Endocr Rev. 2006. https://doi.org/10.1210/er.2006-0020
8. Gupta M, et al. Menopause and hair loss: exploring the hormonal transition. Maturitas. 2025. https://doi.org/10.1016/j.maturitas.2025.108378
9. Drake L, et al. Evaluation of the safety and effectiveness of nutritional supplements for treating hair loss: a systematic review. JAMA Dermatol. 2023. https://doi.org/10.1001/jamadermatol.2022.4867
10. Dasgupta A. Biotin interference in immunoassays. Adv Clin Chem. 2022. https://doi.org/10.1016/bs.acc.2022.03.005
11. Murata K, Noguchi K, Kondo M, et al. Promotion of hair growth by Rosmarinus officinalis leaf extract. Phytother Res. 2013;27(2):212-217. https://doi.org/10.1002/ptr.4712
12. Chéret J, Bertolini M, Ponce L, et al. Olfactory receptor OR2AT4 regulates human hair growth. Nat Commun. 2018;9:3624. https://doi.org/10.1038/s41467-018-05973-0
13. Jimenez F, López E, Bertolini M, et al. Topical odorant application of the specific olfactory receptor OR2AT4 agonist, Sandalore, improves telogen effluvium-associated parameters. J Cosmet Dermatol. 2020;20(3):784-791. https://doi.org/10.1111/jocd.13608
14. Herman A, Herman AP. Caffeine’s mechanisms of action and its cosmetic use. Skin Pharmacol Physiol. 2013;26(1):8-14. https://doi.org/10.1159/000343174
15. Ablon G. A 3-month, randomized, double-blind, placebo-controlled study evaluating the ability of an extra-strength marine protein supplement to promote hair growth and decrease shedding in women with self-perceived thinning hair. Dermatol Res Pract. 2015;2015:841570. https://doi.org/10.1155/2015/841570
16. Rizer RL, Stephens TJ, Herndon JH, et al. A marine protein-based dietary supplement for subclinical hair thinning/loss: results of a multisite, double-blind, placebo-controlled clinical trial. Int J Trichology. 2015;7(4):156-166. https://doi.org/10.4103/0974-7753.171573
17. Yorulmaz A, Hayran Y, Ozdemir AK, et al. Telogen effluvium in daily practice: patient characteristics, laboratory parameters, and treatment modalities of 3028 patients. J Cosmet Dermatol. 2021;21(6):2610-2617. https://doi.org/10.1111/jocd.14413
18. Siah TW, Muir-Green L, Shapiro J. Female pattern hair loss: a retrospective study in a tertiary referral center. Int J Trichology. 2016;8(2):57-61. https://doi.org/10.4103/0974-7753.188033
19. SUHS / Sonoran University naturopathic clinical training, Alopecia clinical protocol (Dr. Shad Abdulla, ND). [Naturopathic training: silicon-rich foods, scalp massage, anti-inflammatory diet, tier-labeled as traditional support without regrowth trials.]