Does Gluten-Free Really Lower Hashimoto’s Antibodies?
Have you been told that cutting gluten will drop your thyroid antibodies and quiet your Hashimoto’s? Here is the honest answer. The trials do not show that gluten-free reliably lowers thyroid antibodies in people who have Hashimoto’s but not celiac disease. Some women still get real digestive relief, which is a separate question from the thyroid.
I am Dr. Shad Abdulla, ND, and I read the actual studies before I say anything about them. Most of the loudest voices on this topic skip the one thing that matters. So let me back up. I will walk you through what the evidence really says, who gluten-free actually helps, and how to test it for yourself safely. By the end you will have a clear decision path you can save.
A quick word on terms. Hashimoto’s is an autoimmune condition where your immune system slowly attacks the thyroid, the small gland in your neck that sets your energy and metabolism. Anti-TPO and anti-Tg are antibodies, meaning immune proteins your body makes against your own thyroid tissue, and doctors measure them in your blood. Keep those two words in mind, because the whole debate turns on them.
Does cutting gluten actually lower your thyroid antibodies?
No, the trials do not show that gluten-free reliably lowers thyroid antibodies in non-celiac Hashimoto’s. This is the part the wellness world leaves out, and it is the most important thing on this page.
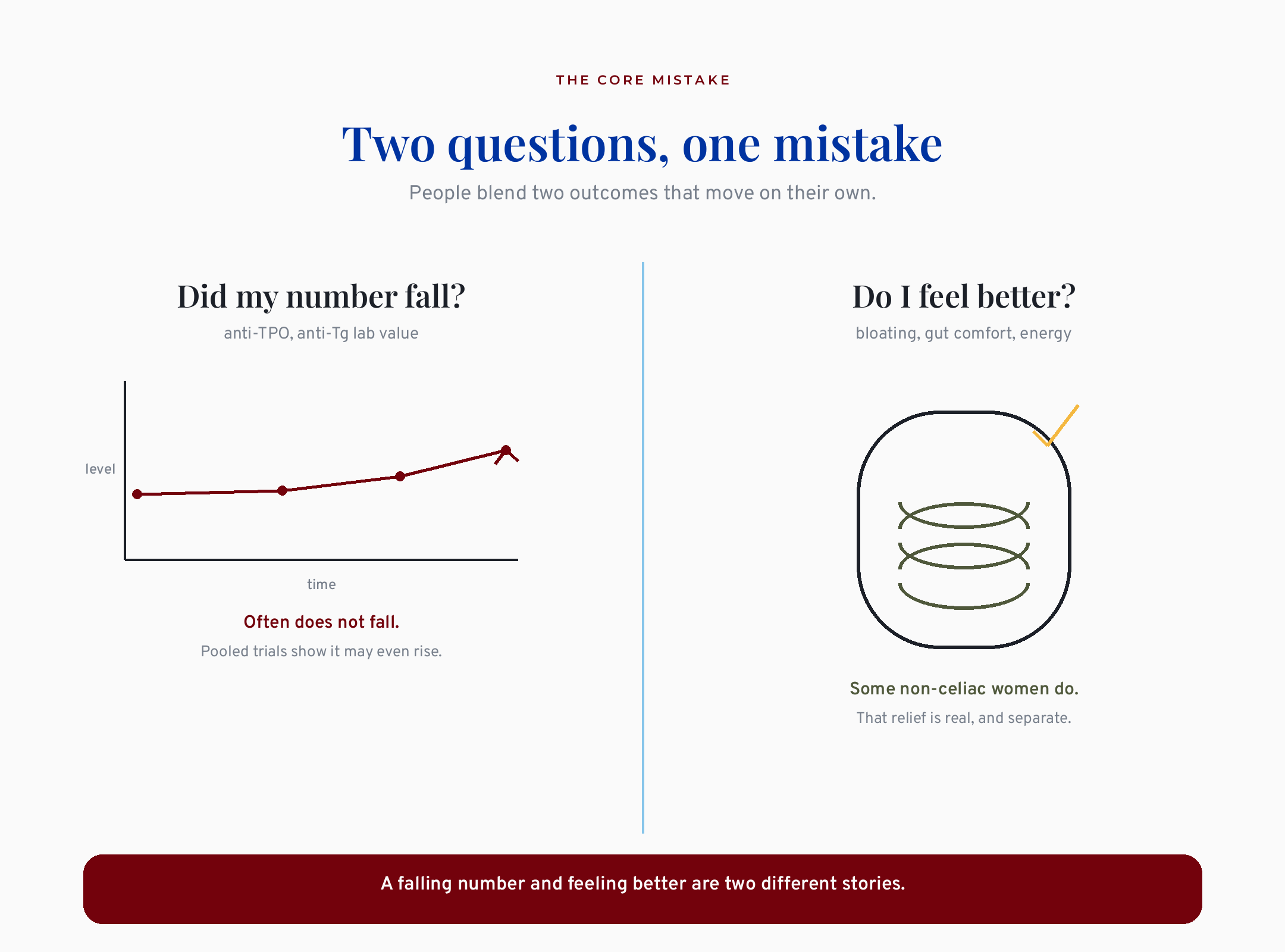
Split diagram contrasting whether Hashimoto’s thyroid antibodies fall versus whether gut symptoms improve on gluten-free
Here is where it gets uncomfortable for the popular story. A 2025 meta-analysis of 110 patients found gluten-free raised anti-TPO antibodies, not lowered them (Araujo 2025). A meta-analysis is a study that pools several trials together to see the overall pattern. This one looked only at randomized trials, the most rigorous kind, and the anti-TPO number went up, not down. The same analysis found anti-Tg fell a little, and it found no change at all in your actual thyroid hormone levels.
I want to be fair to the whole picture, because honesty cuts both ways. The anti-Tg drop is real and it shows up in more than one analysis, so I am not going to pretend it does not exist. But it is small, it sits next to a rise in the other antibody, and thyroid function did not change. That is not the clean “gluten lowers your antibodies” win you have been sold.
What this means for the woman in front of me is simple. If you go gluten-free hoping to watch your antibody number fall, the evidence says do not count on it. That does not make your symptoms imaginary. It just means the number and the feeling are two different stories.
Bottom line so far: the most rigorous pooled trial data show gluten-free does not reliably drop your thyroid antibodies, and may nudge anti-TPO up.
What does the longest, strongest study show?
The single longest trial followed women for a full year and found no antibody benefit from gluten-free. That length matters, because most diet studies run only six or eight weeks, which is barely enough time to see a slow autoimmune process shift.
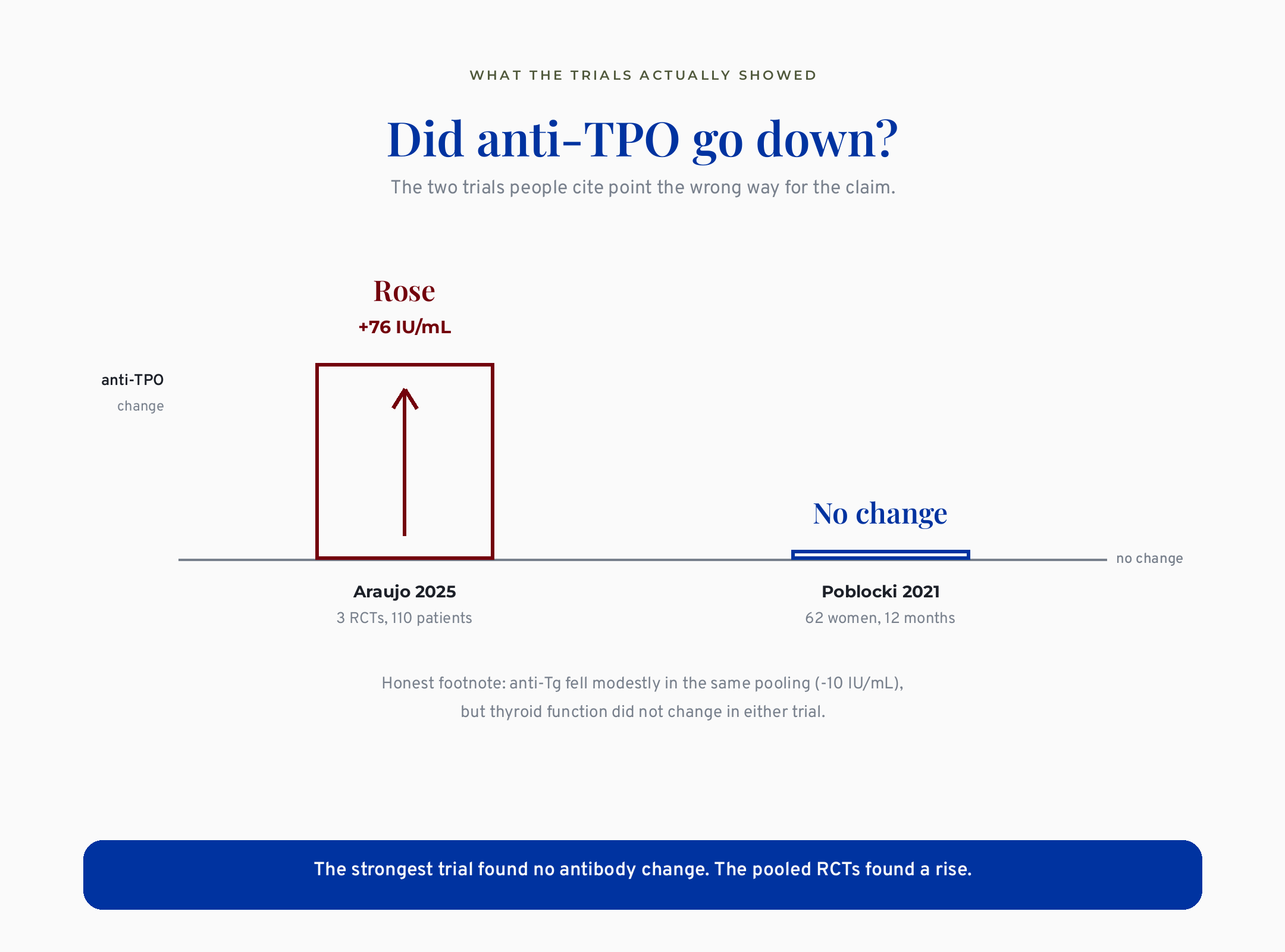
Bar comparison of anti-TPO change on gluten-free, rising 76 in Araujo 2025 versus no change in Poblocki 2021
The longest trial, 62 women over 12 months, found gluten-free changed no thyroid antibody at all (Poblocki 2021). These were women with autoimmune thyroiditis who had celiac ruled out first. After a year of careful gluten avoidance, neither anti-TPO nor anti-Tg moved between the groups. Their TSH did drop a little. TSH, meaning thyroid-stimulating hormone, is the brain’s signal telling the thyroid to work harder, so a lower number can look encouraging. But TSH alone is not the same as the disease retreating, and the antibodies that define Hashimoto’s stayed put.
A cleaner test came a few years later. A 2025 trial compared three diets head to head. Gluten-free changed nothing on antibodies or thyroid function. Only the Mediterranean diet improved markers of oxidative stress, meaning cellular wear and tear. Read that twice. A non-elimination diet outperformed the elimination diet that everyone online is pushing.
I think about the woman who already cut bread, pasta, and the foods tied to her family table. She got nothing back on her labs. The research says she is not alone, and she did not do it wrong. The longest and cleanest trials point the same direction: gluten removal does not move the antibodies, and a gentler eating pattern may do more.
Then why does everyone online say gluten is the root cause?
Because the mechanism sounds convincing, and one early study gave the story a foothold. Let me explain both, because you deserve to know why a claim spread, not just that it did.
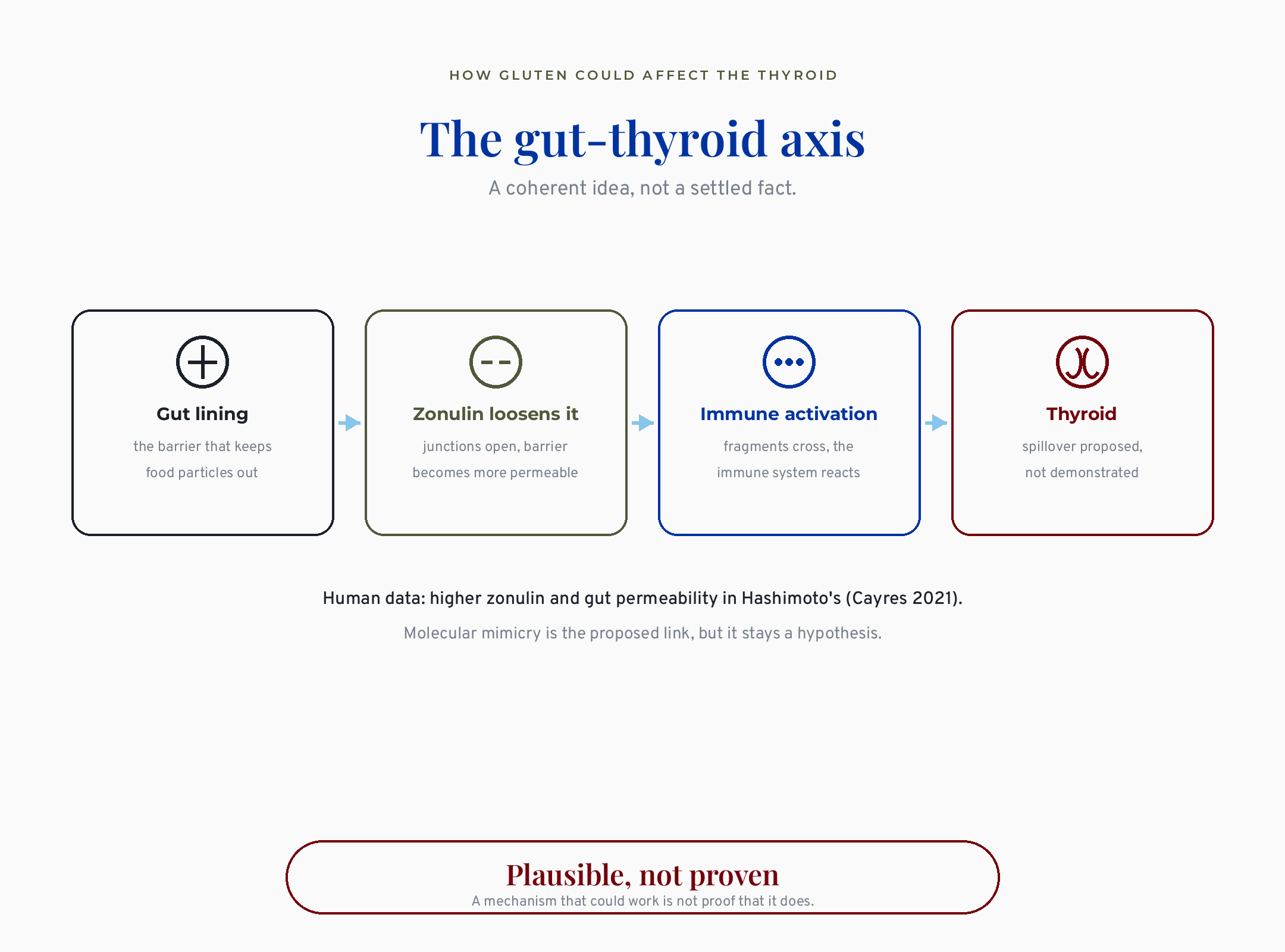
Gut-thyroid axis showing zonulin loosening the gut barrier then immune activation, labeled plausible not proven
The mechanism goes like this. In Hashimoto’s, the gut lining can become more permeable, meaning the barrier that normally keeps food particles out of the bloodstream gets a little leaky. Researchers measure this partly through zonulin, a protein that loosens the junctions between gut cells. The idea is that a leaky barrier lets gluten fragments trigger an immune reaction that spills over to the thyroid. There is real human data showing higher zonulin in Hashimoto’s patients. So the gut-thyroid connection is plausible.
Here is the catch I want you to hold onto. A mechanism that could work is not proof that removing gluten does work. One careful review put it plainly: gluten-free does not reverse the autoimmune process already established in the gland. Plausible is not the same as proven, and the science writers who say “molecular mimicry is settled” are getting ahead of the data.
The foothold is one Polish pilot study of 34 drug-naive women. It did show lower antibodies, but only in a selected subgroup who tested positive for an anti-tTG marker. It was small, it was never replicated, and it came from a single center. That one study gets cited everywhere because it is the rare positive result in a field of nulls.
What this means for you is that the confident “root cause” story rests on a hopeful mechanism plus one unrepeated pilot. That is a thin foundation for a permanent diet change. The gut-barrier idea is real biology, but it is a hypothesis, not the settled root-cause fact you keep hearing.
What does conventional medicine get wrong here?
Conventional medicine gets the science mostly right and the woman mostly wrong. It correctly says no diet reverses Hashimoto’s and that levothyroxine comes first. Levothyroxine is the standard thyroid hormone replacement medication, meaning a pill that supplies the hormone your gland is no longer making enough of. On the evidence, the guideline bodies are not wrong about that.
Where the conventional side fails is the person. It tells a woman whose labs look fine that there is nothing to discuss, then sends her home still exhausted, still bloated, still not herself. That flat dismissal is exactly why she ends up on TikTok at midnight, because at least someone there is taking her seriously.
This is the real root-cause work that gets skipped. It means looking at the whole person. The gut, the nutrient gaps, and the symptoms that persist even when the thyroid number looks normal all belong in the conversation. That is the naturopathic instinct done right. It does not mean blaming one food for everything. It means refusing to stop the conversation at “your labs are normal.”
I have seen this whiplash play out in cases I have reviewed. A primary care doctor says go gluten-free. An endocrinologist says it is unnecessary. The woman is left holding two opposite instructions and a lot of self-doubt. Both doctors are partly right. Conventional medicine is right that diet does not reverse the disease. It is wrong to treat a dismissed, symptomatic woman as if her experience does not count.
So who actually benefits from going gluten-free?
A specific group benefits clearly, and a larger group might benefit for reasons that have nothing to do with their thyroid. Sorting yourself into the right group is the whole game, and almost no one online does it for you.
The clear case is celiac disease. Celiac is an autoimmune reaction to gluten that damages the small intestine, and people with Hashimoto’s have a higher chance of having it. If you have celiac, gluten-free is genuinely necessary and permanent, full stop. Untreated celiac can even raise the dose of thyroid medication you need, because a damaged gut absorbs the pill poorly. This is why testing comes first.
The maybe case is the woman without celiac who has ongoing gut symptoms. Some people without celiac do report real digestive relief off gluten, meaning less bloating and discomfort, even though their thyroid antibodies do not budge. That relief is legitimate. It is just a gut story, not a thyroid story, and conflating the two is what leads to disappointment when the lab comes back unchanged.
The third group is the true non-responder. She cuts gluten, tracks it honestly, and nothing changes, not her gut and not her labs. For her, continuing is cost and restriction with no payoff, and stopping is not a failure. If your gut is part of why you feel off, my deep dive on SIBO subtypes and why they relapse may help more.
What this means for the woman in front of me is that “everyone with Hashimoto’s should quit gluten” is too blunt to be useful. Celiac is the clear yes, ongoing gut symptoms are a reasonable maybe, and a clean non-response is a fair no.
So what actually helps, beyond removing gluten?
This is the part the gluten-only conversation skips, and it is the part I care about most as a naturopathic doctor. My root-cause lens does not mean I reach for a supplement first. It means I ask what is actually worth adding before anyone reaches for anything. So here is the honest toolkit, sorted by how strong the evidence really is. None of this is a prescription. It is education, and every one of these is a conversation to have with your own clinician, because that is your doctor’s call, not a blog’s.
The options with real trial support
Selenium. This is the one with the most support, and it is stronger than gluten removal. Selenium is a trace mineral your thyroid needs to handle oxidative stress, meaning cellular wear and tear. Two meta-analyses found that supplementing it significantly lowered thyroid antibodies (Toulis 2010, Wichman 2016), and the newest and largest pooling, 21 trials and 1,610 people, found the same drop in TPO antibodies at three and six months (Zhang 2025). The honest caveat is the same one I keep repeating: lowering an antibody is not proven to change how you feel, so I hold even this loosely. And here is the irony the gluten-free story misses. Wheat is a real dietary source of selenium, so going gluten-free can quietly lower the very nutrient with better thyroid evidence than gluten removal itself.
Myo-inositol with selenium. For one specific group, this combination did more than selenium alone. If your thyroid is just starting to slip, meaning subclinical hypothyroidism where your TSH is mildly raised but your thyroid hormones are still normal, adding myo-inositol, a sugar-like compound your thyroid uses for signaling, to selenium lowered TSH and both antibodies and improved how people felt in a trial of 168 patients (Nordio 2017). A 2026 pooling confirmed the TSH benefit while urging caution on the antibody numbers (Stanchev 2026). Promising, still a small evidence base.
Vitamin D. Worth checking if your level is actually low. Pooled trials found vitamin D lowered TPO antibodies, though it did not change thyroid function (Jiang 2022). The move here is to correct a real deficiency, not to megadose chasing the antibody number.
The eating pattern with more support than elimination
Here is the quiet finding the headlines miss. In that head-to-head trial I mentioned, it was the Mediterranean pattern, not gluten removal, that actually moved a marker, lowering oxidative stress (Lagana 2025). So if you are going to change how you eat, the better-supported move is adding, more vegetables, olive oil, fish, fiber, rather than subtracting one protein. And if your real goal is how you feel day to day, there is an honest option for that too. The Autoimmune Protocol, a structured phased elimination-and-reintroduction diet, improved quality of life and cut symptom burden sharply in Hashimoto’s women, even though it did not move their antibodies or thyroid function (Abbott 2019). That is the same split as gluten-free, said plainly: it may help how you feel, not what the lab says. This is also where the gut-thyroid work belongs, including the nutrient overlap that gets missed, especially iron, which sits at the crossroads of fatigue and thyroid symptoms. I wrote about that in iron deficiency without anemia and the fatigue it causes, because so many women get told their iron is fine when their ferritin tells a different story.
Traditional support, named honestly
Ashwagandha. This is one I hold gently and respectfully. Ashwagandha is a plant used in Ayurvedic medicine for the thyroid for a very long time, and in one small trial of 50 people with a mildly underactive thyroid, 600 mg a day improved thyroid hormone levels against placebo (Sharma 2018). I have real respect for the plant and the tradition behind it. I will also be straight with you about the tier it sits in: it was one small pilot, it was not Hashimoto’s specifically, and it was not measured against your antibodies. It can nudge thyroid hormones upward, so it is a clinician-supervised option, not a casual one. Traditionally used and early-promising is the honest label, not proven.
Two things from my own training worth knowing
A small reassurance first. You do not have to give up cruciferous vegetables. Raw broccoli, cabbage, and kale contain goitrogens, compounds that can mildly interfere with the thyroid, but cooking deactivates most of them. So you cook them, you do not banish them. That is the kind of detail I learned in my naturopathic training that gets flattened into an all-or-nothing rule online.
And one honest disagreement inside my own field, because honesty inside naturopathic medicine matters as much as honesty about it. A lot of traditional naturopathic teaching, including the protocols I studied in school, recommends iodine and sea vegetables like kelp for thyroid support. The newer evidence points the other way for Hashimoto’s specifically: too much iodine can actually fuel the autoimmune attack. So here is where I land, and I will tell you plainly that not every naturopath agrees with me. Favor selenium and food-first minerals, and be cautious with high-dose iodine and kelp when the problem is Hashimoto’s.
The honest read is that real options exist beyond removing gluten: selenium has the best trial support, myo-inositol-plus-selenium and vitamin D help specific groups, a Mediterranean pattern beat elimination head to head, the Autoimmune Protocol can lift how you feel without moving the antibody number, and traditional botanicals like ashwagandha are worth knowing and worth tiering honestly.
What are the real downsides of going gluten-free if you do not need it?
Going gluten-free is not a free experiment, and treating it as harmless is its own kind of dishonesty. If you need it for celiac, the trade-offs are worth it. If you do not, they still apply.
The first cost is nutritional. Gluten-free substitute products tend to be lower in fiber and several nutrients and higher in fat. Removing wheat removes a real source of fiber, B vitamins, and iron. For a menstruating woman or one moving through perimenopause, those iron and folate gaps are not trivial. The second cost is literal. Gluten-free products are more expensive, and the bill adds up over months of strict avoidance.
There is a subtler one most people never mention. Many gluten-free products lean on rice flour, and rice naturally takes up arsenic from soil. One prospective study found urinary arsenic rose roughly four-fold after people adopted a gluten-free diet. The levels were not acutely dangerous, but the long-term meaning is simply unknown, because no one has studied non-celiac adults on gluten-free for years.
The last one is the most human. Strict food rules can tip toward disordered eating in someone already prone to it. The constant vigilance around cross-contamination can become its own source of stress. For a woman whose relationship with food is already strained, that risk deserves to be named out loud, not waved away.
What this means for the woman in front of me is that the decision is not “try it, what do you have to lose.” There is something to lose, so the experiment should be deliberate. An unneeded gluten-free diet can cost you fiber, nutrients, money, and peace around food, with arsenic from rice products as a real and understudied wrinkle.
What I’d do this week
If you want to test gluten-free for yourself, do it like a clean experiment. Give it a beginning, an end, and a rule you decide in advance. Here is the path I would save and follow, and I would not skip a single step.
A note on confidentiality before the card. The patterns below come from cases I have reviewed and women I have worked with, with identifying details changed to protect privacy. Take this as education, not a prescription for your specific body.
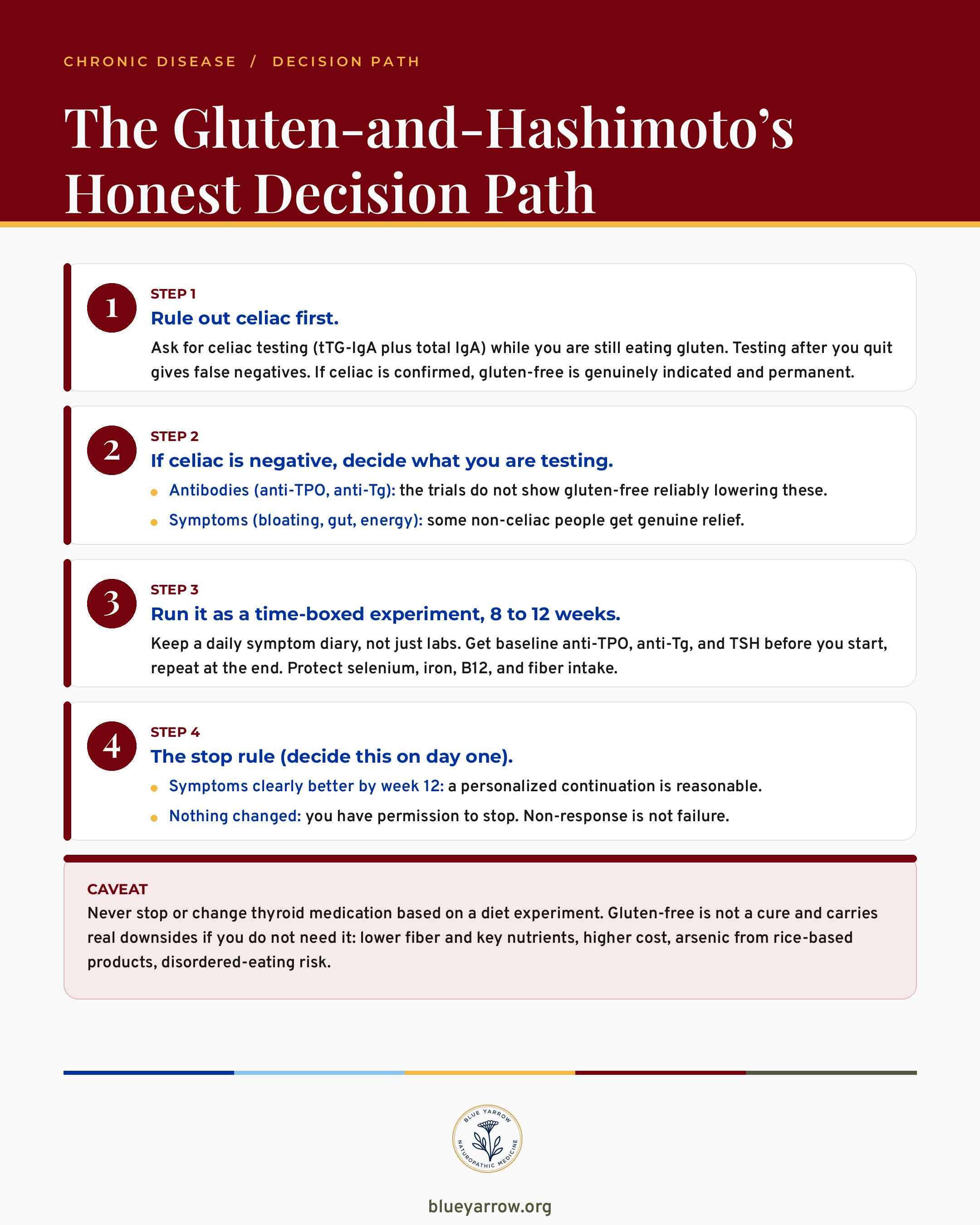
The takeaway in one line: rule out celiac, pick what you are testing, run a tracked 8-to-12-week trial, and set your stop rule first.
How honest is the evidence, really?
It is honest to admit the trial base here is small, short, and a little messy. I would rather tell you that than pretend the science is settled in either direction.
Most of these studies enrolled a few dozen people and ran for months, not years. Many of the null trials never confirmed that participants actually stayed off gluten. A real effect in strictly compliant people could be hiding under that non-compliance noise. The single positive antibody signal sits in one unreplicated subgroup from one center. And nobody has shown that an antibody change, up or down, tracks with how a woman actually feels.
So the fair verdict is not “gluten-free does nothing for anyone.” It is that gluten-free does not reliably move thyroid antibodies or function in non-celiac Hashimoto’s. Celiac is the real exception, and some people get genuine gut relief. The evidence is weak and mixed, which is exactly why a tracked personal experiment beats a blanket rule.
Quote card reading a 2025 meta-analysis of 110 patients found gluten-free raised anti-TPO antibodies, not lowered them
Quote card reading a 2025 meta-analysis of 110 patients found gluten-free raised anti-TPO antibodies, not lowered them
Sorting out overlapping thyroid and hormone labs? My post on the Hashimoto’s and PCOS thyroid panel walks through which numbers are actually worth asking your doctor for.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Frequently asked questions
Does gluten-free lower thyroid antibodies in Hashimoto’s? The randomized trials do not show gluten-free reliably lowering thyroid antibodies in people who have Hashimoto’s without celiac disease. The most rigorous pooled analysis actually found anti-TPO rising. Anti-Tg fell a little in some data, but thyroid function did not improve.
Do I have to go gluten-free if I have Hashimoto’s but not celiac? No guideline recommends gluten-free for non-celiac Hashimoto’s. If you have ongoing gut symptoms, a tracked 8-to-12-week trial is reasonable to test for digestive relief. Just separate that gut question from your thyroid antibodies, which the trials say are unlikely to move.
How long before gluten-free shows a change? The longest trial ran a full year and still found no antibody change. If you are testing for gut symptoms, most people who respond notice it within 8 to 12 weeks. That window is why a time-boxed experiment with a clear stop rule makes more sense than open-ended avoidance.
Should I get tested for celiac before quitting gluten? Yes, and this order matters. Ask for tTG-IgA plus total IgA while you are still eating gluten, because testing after you stop produces false negatives. People with Hashimoto’s have a higher chance of celiac, and a positive result changes everything, since gluten-free is then genuinely necessary.
Is going gluten-free safe if I do not need it? It is not risk-free. An unneeded gluten-free diet can lower fiber, iron, B12, and selenium, costs more, and relies on rice products that raise arsenic exposure. It can also strain your relationship with food. None of that means do not try it, only that it deserves a deliberate plan.
Will gluten-free reverse my Hashimoto’s? No diet reverses Hashimoto’s, and thyroid hormone replacement remains first-line care. Reviews are clear that gluten removal does not undo the autoimmune process already in the gland. A falling antibody number, if you ever see one, is not proof the disease is gone.
If gluten-free is not the answer, what actually helps Hashimoto’s? Several things have better evidence than gluten removal, and it is a disservice to lump them together. Selenium has the strongest antibody support across meta-analyses (Toulis 2010, Wichman 2016, Zhang 2025). For a mildly underactive thyroid, myo-inositol with selenium lowered TSH and antibodies (Nordio 2017), and vitamin D lowers TPO antibodies if you are deficient (Jiang 2022). A Mediterranean pattern outperformed gluten-free head to head (Lagana 2025), and the Autoimmune Protocol diet improved quality of life and symptoms even though it did not move antibodies (Abbott 2019). Ashwagandha has traditional use and one small pilot trial (Sharma 2018), so I tier it as promising, not proven. All of this is education to discuss with your clinician, not a prescription.
References
1. Araujo, E. M. Q., Coutinho-Lima, C. R. O., Sousa, A. S., et al. (2025). Effects of gluten-free diet in non-celiac Hashimoto’s thyroiditis: A systematic review and meta-analysis. Nutrients, 17(21), 3437. https://doi.org/10.3390/nu17213437
2. Poblocki, J., Panka, T., Szczuko, M., Telesinski, A., & Syrenicz, A. (2021). Whether a gluten-free diet should be recommended in chronic autoimmune thyroiditis or not? A 12-month follow-up. Journal of Clinical Medicine, 10(15), 3240. https://doi.org/10.3390/jcm10153240
3. Piticchio, T., Frasca, F., Malandrino, P., et al. (2023). Effect of gluten-free diet on autoimmune thyroiditis progression in patients with no symptoms or histology of celiac disease: A meta-analysis. Frontiers in Endocrinology, 14, 1200372. https://doi.org/10.3389/fendo.2023.1200372
4. Lagana, A., Piticchio, T., Alibrandi, A., Le Moli, R., et al. (2025). Effects of dietary habits on markers of oxidative stress in subjects with Hashimoto’s thyroiditis: Mediterranean versus gluten-free diet. Nutrients, 17(2), 363. https://doi.org/10.3390/nu17020363
5. Pu, X., Long, Y., Yue, Y., Zhang, X., Jiang, H., & Li, X. (2025). Autoimmune thyroid diseases, celiac disease and gluten-free diet: A Mendelian randomisation study. British Journal of Nutrition. https://doi.org/10.1017/S0007114525103917
6. Krysiak, R., Szkrobka, W., & Okopien, B. (2018). The effect of gluten-free diet on thyroid autoimmunity in drug-naive women with Hashimoto’s thyroiditis: A pilot study. Experimental and Clinical Endocrinology & Diabetes. https://doi.org/10.1055/a-0653-7108
7. Cayres, L. C. F., et al. (2021). Detection of alterations in the gut microbiota and intestinal permeability in patients with Hashimoto thyroiditis. Frontiers in Immunology, 12, 579140. https://doi.org/10.3389/fimmu.2021.579140
8. Kahaly, G. J., Frommer, L., & Schuppan, D. (2018). Celiac disease and glandular autoimmunity. Nutrients, 10(7), 814. https://doi.org/10.3390/nu10070814
9. Toulis, K. A., et al. (2010). Selenium supplementation in the treatment of Hashimoto’s thyroiditis: A systematic review and meta-analysis. Thyroid, 20(10). https://doi.org/10.1089/thy.2009.0351
10. Wichman, J., et al. (2016). Selenium supplementation significantly reduces thyroid autoantibody levels in patients with chronic autoimmune thyroiditis: A systematic review and meta-analysis. Thyroid, 26(12). https://doi.org/10.1089/thy.2016.0256
11. de la Calle, I., et al. (2020). Celiac disease: Nutritional assessment of the gluten-free diet. Nutricion Hospitalaria. https://doi.org/10.20960/nh.02913
12. Du, S., et al. (2024). Arsenic exposure after adopting a gluten-free diet: A prospective cohort. American Journal of Gastroenterology. https://doi.org/10.14309/ajg.0000000000003117
13. Motazedian, N., et al. (2023). Metabolic syndrome after one year of a gluten-free diet. Middle East Journal of Digestive Diseases. https://doi.org/10.34172/mejdd.2023.342
14. Zhang, H., Yang, Y., Liu, S., Yang, Y., & Liu, Z. (2025). Clinical efficacy of selenium supplementation in patients with Hashimoto thyroiditis: A systematic review and meta-analysis. Medicine (Baltimore), 104(35), e44043. https://doi.org/10.1097/MD.0000000000044043
15. Nordio, M., & Basciani, S. (2017). Myo-inositol plus selenium supplementation restores euthyroid state in Hashimoto’s patients with subclinical hypothyroidism. European Review for Medical and Pharmacological Sciences, 21(2 Suppl), 51-59. PMID 28724185
16. Stanchev, P., Kraeva, M., Petrov, P., & Penchev, P. (2026). Myo-inositol plus selenium vs. selenium alone in Hashimoto’s thyroiditis with subclinical hypothyroidism: A systematic review and updated meta-analysis. Journal of Clinical Medicine, 15(9), 3179. https://doi.org/10.3390/jcm15093179
17. Jiang, H., Chen, X., Qian, X., & Shao, S. (2022). Effects of vitamin D treatment on thyroid function and autoimmunity markers in patients with Hashimoto’s thyroiditis: A meta-analysis of randomized controlled trials. Journal of Clinical Pharmacy and Therapeutics, 47(6), 767-775. https://doi.org/10.1111/jcpt.13605
18. Abbott, R. D., Sadowski, A., & Alt, A. G. (2019). Efficacy of the Autoimmune Protocol diet as part of a multi-disciplinary, supported lifestyle intervention for Hashimoto’s thyroiditis. Cureus, 11(4), e4556. https://doi.org/10.7759/cureus.4556
19. Sharma, A. K., Basu, I., & Singh, S. (2018). Efficacy and safety of ashwagandha root extract in subclinical hypothyroid patients: A double-blind, randomized placebo-controlled trial. Journal of Alternative and Complementary Medicine, 24(3), 243-248. https://doi.org/10.1089/acm.2017.0183
20. SUHS / Sonoran University naturopathic clinical training, Hashimoto’s thyroiditis treatment protocols (Dr. Shad Abdulla, ND). [Naturopathic clinical training, traditional-use and clinical depth: cooking goitrogenic foods, thyroid trace minerals, the iodine-restriction nuance.]