Why Your SIBO Keeps Coming Back (And What Actually Helps)
If you have ever had SIBO, you already know how exhausting this gets. You did the protocol. You took the antibiotic, or the herbal blend, or both. You retested. And then it came back, and nobody warned you it would. That is not a personal failure, and it is not in your head. In cases I have reviewed, this exact loop is the rule, not the exception. Here is the promise of this piece. I will show you why relapse happens, why your subtype label is not the answer you were sold, and what actually changes the odds. You will get the four drivers I keep coming back to, the one most doctors skip, and a save card you can bring to your next appointment. Let me back up a little and explain what is really going on.
Why does my SIBO keep coming back after treatment?
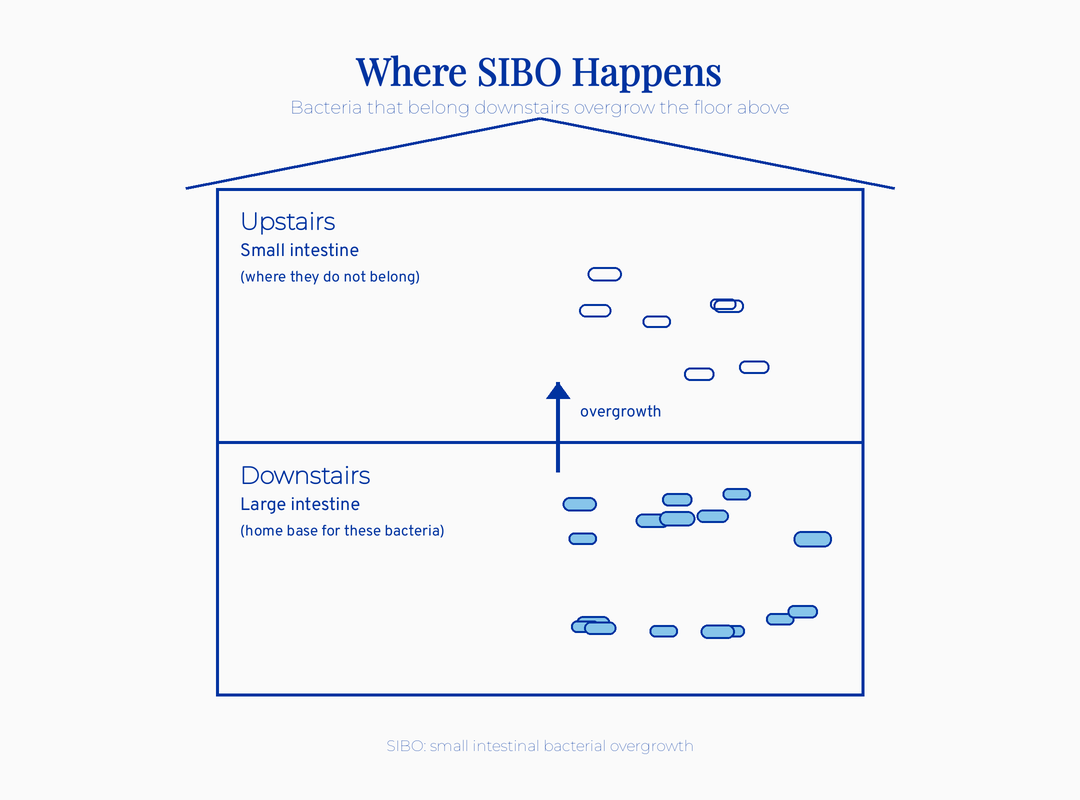
Your SIBO keeps coming back because the upstream driver was never addressed, not because the antibiotic failed. That is the single most important sentence in this article. You cleared the bacteria. You did your part. The problem is that clearing bacteria and fixing the reason they overgrew are two different jobs. Most protocols only do the first one. Let me define the term so the map is clear. SIBO stands for small intestinal bacterial overgrowth. The plain-language version is that bacteria which belong downstairs in your large intestine set up shop on your second floor. That second floor is your small intestine, where they do not belong. So they ferment your food too early. You feel it as bloating, pain, and changes in how you go to the bathroom.
Here is the number that names your experience. Rifaximin clears SIBO in up to 71% of people, but 44% relapse by nine months (Gatta 2017). Rifaximin is a gut-specific antibiotic that stays mostly inside your intestine instead of being absorbed into your bloodstream.
So the kill works. The holding does not.
The short version. Eradication is common and durable remission is rare. Relapse is a signal that something upstream is still open, not proof that you did anything wrong.
Does my SIBO type actually change my treatment?
Your subtype matters in one specific way, and the wellness industry has oversold the rest. The methane pattern points you toward motility. Beyond that, the precise hydrogen-versus-sulfide sorting does not reliably change outcomes in the research.
You were probably handed a label. Hydrogen type. Methane type. Maybe a third gas. Let me explain what those mean and where the line of honest evidence actually sits.
The methane pattern now has its own name, IMO, which stands for intestinal methanogen overgrowth. IMO is not even a bacterial problem. It is an overgrowth of an archaeon, a different class of microbe, that produces methane gas.
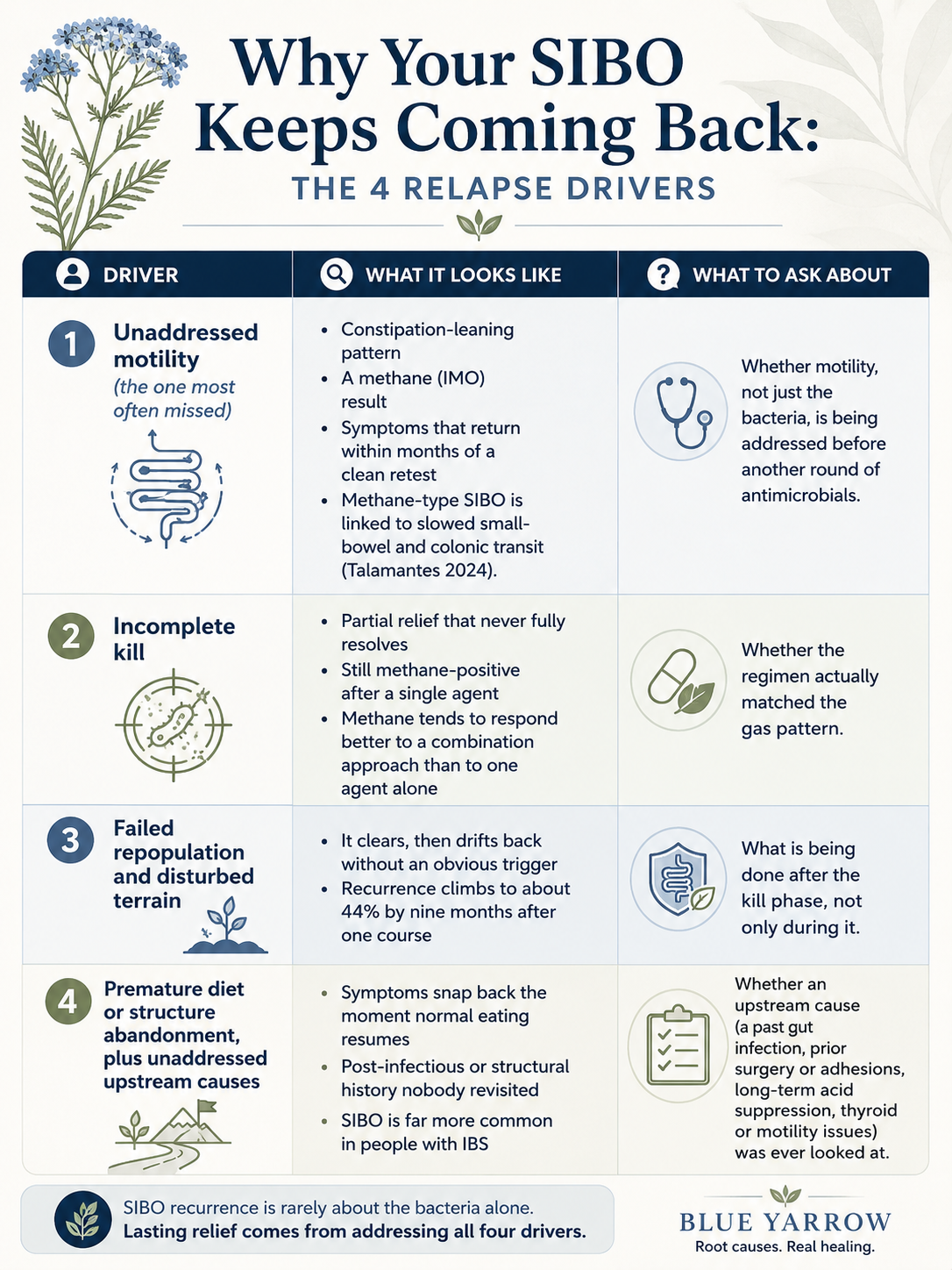
That detail is not trivia. Methane-type SIBO slows gut transit, with colonic transit of 44 versus 29 hours (Talamantes 2024). Transit is simply how long it takes food to move through you.
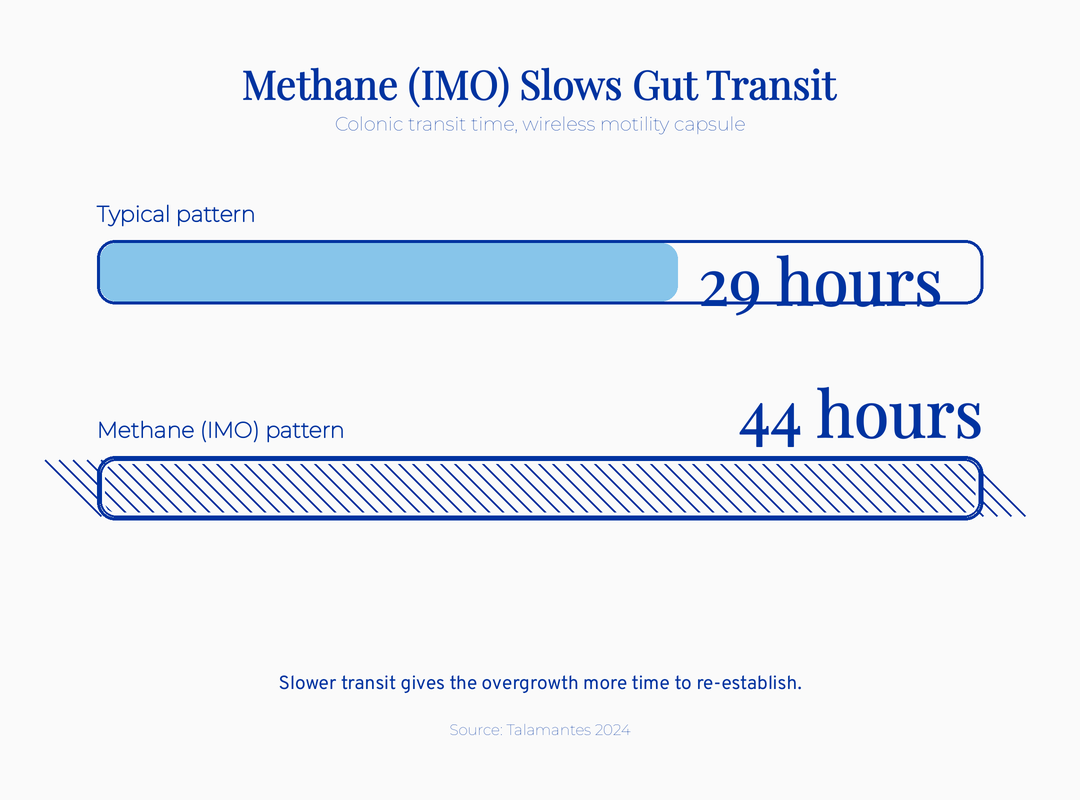
Slow transit gives the overgrowth more time to re-establish itself. That is why this pattern leans toward constipation. It is also why it returns when nobody addresses the slowdown.
The root-cause version of this question is not “which gas am I.” It is “what is keeping the door open.” A woman I worked with had cycled through two clean retests and still relapsed both times, because her constipation, the actual slowdown, was never on the treatment plan. What this means for the woman in front of me is simple. The label is a clue about mechanism, not a destination.
The micro-summary. Use your subtype to find the mechanism, especially a methane result pointing at slowed motility. Do not treat the label as a precise diagnosis or a cure path.
What is the most common reason SIBO relapses?
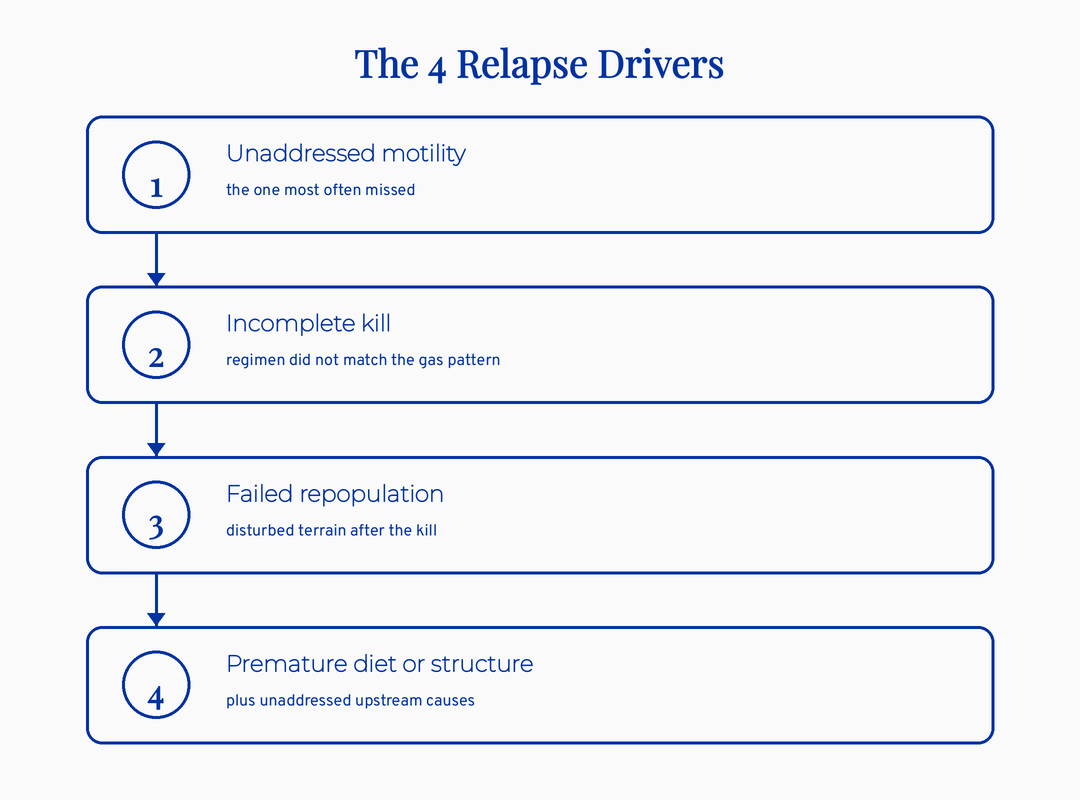
Slowed motility is the relapse driver I see missed most often. Motility is the wave of muscle contractions that sweeps your small intestine clean between meals, like a janitor that runs the halls when everyone has gone home. When that sweep slows down, bacteria linger and regrow, no matter how good the kill was.
This is where the methane finding earns its keep. The transit data ties the methane pattern directly to a mechanical problem, not just a microbial one. A prokinetic is a medication or agent that speeds that cleaning wave back up. In the comparative research, a prokinetic ranks highest when a motility or functional-gut problem is also present.
Here is a position I hold firmly. Prokinetics treat downstream. We have to look upstream first. That is the difference between chasing the gas and fixing the slowdown that lets the gas come back.
What this means for the woman in front of me. If your pattern leans toward constipation and a methane result, the motility question deserves to be on the table before another round of antimicrobials.
Did my past antibiotics cause this?
This is the hardest and most honest part, so I want to be careful. Repeated antimicrobial rounds may reshape the gut environment in ways that leave it more vulnerable to the next overgrowth. I call this the antibiotic paradox. The same tool that clears the overgrowth may, used over and over, be part of what keeps the terrain hospitable to it.
I want to be clear about what this is not. This is not anti-medicine. Antibiotics are a legitimate, often necessary tool, and a single well-chosen course is not the villain here. The honest tension is about cycling the same approach endlessly and expecting a different result.
There is no good long-term safety data on repeated antimicrobial cycling, whether the agent is pharmaceutical or herbal. So I will not reassure you that doing it again and again is harmless, because the research does not let me. What I want you to understand is that “kill it again” is not a neutral act. It carries a cost the research cannot yet fully measure.
The micro-summary. A single targeted course is a reasonable tool. Endless repeat rounds, without a plan for what comes after the kill, may quietly work against you.
What if I was told it is just IBS?
If you carry an IBS label, a treatable overgrowth may be hiding underneath it. This is one of the most common patterns I see in the research, and it reframes the whole story. IBS stands for irritable bowel syndrome, a diagnosis given when the gut misbehaves but standard tests look clean. The trouble is that the label describes the symptoms without naming the cause.
Here is the link that matters. SIBO is far more common in people with IBS than in people without it, with the odds running several times higher in the pooled research. So a meaningful share of women told they have IBS may be living with an untreated or relapsing SIBO component.
That does not mean every IBS diagnosis is secretly SIBO. It means the question deserves to be asked rather than waved off.
Think of one woman I worked with in cases I have reviewed. She had carried an IBS label for years, cycled through fiber, then a low-FODMAP diet, then nothing, with no lasting relief. Her bloating got worse the longer each day went on, which is a motility pattern, not a random one. The IBS label had quietly closed a door that needed reopening.
What this means for the woman in front of me. An IBS diagnosis is a starting line, not a finish line. If your pattern fits, asking whether an overgrowth is part of the picture is a fair and useful question.
Are herbal antimicrobials safer or better than antibiotics?
Herbal antimicrobials performed comparably to the antibiotic in one head-to-head study, with fewer reported side effects, but “natural” does not mean “safe for everyone.” Both halves of that sentence matter. Here is the data. Herbal antimicrobials cleared SIBO in 46% versus rifaximin’s 34% in one head-to-head trial (Chedid 2014).
Read that result with care. It was a single open-label trial, which means the participants knew what they were taking. The difference was also not large enough to call herbal superior.
The honest read is that herbal blends look comparable, not magic. The early signal is encouraging, and it is not settled.
Now the safety frame, which is non-negotiable for the women I write for. Berberine and oregano oil are contraindicated in pregnancy and lactation. Berberine can cross the placenta and carries real medication interactions, including with metformin and certain statins. If you are pregnant, trying to conceive, breastfeeding, or on regular medications, “it’s just an herb” is exactly the wrong assumption.
What this means for the woman in front of me is that the herb-versus-drug question is the wrong frame. The approach I find most defensible in the literature is a sequence, not a side. A pharmaceutical agent has a role in the kill phase. Herbal antimicrobials have a role as gentler maintenance for some people.
The right tool depends on your pregnancy intention, your medications, and your history. That is exactly why no honest version of this comes as a one-size dose.
The micro-summary. Herbal blends are a real option, not a safe-for-everyone default. Screen every botanical against pregnancy, lactation, and your medication list first.
What should happen after the kill, not just during it?
The work after the kill is what protects you from relapse, and it is the part most protocols skip. You did the eradication. Now the question is whether anything is in place to keep the small intestine from filling back up. The naturopathic lens on this is that the kill phase buys you a window, and the window closes if nothing changes upstream.
Here is what conventional medicine often misses. A clean retest gets treated as the finish line, when it is closer to the starting line for the part that actually holds. Recurrence climbs to about 44% by nine months after one course, and that curve is not random. It tends to track the drivers that were left unaddressed, especially motility and a disturbed gut environment.
So what fills the window matters. For some people that is motility support so the cleaning wave keeps running. For others it is gentler maintenance, attention to the spacing of meals, or finally evaluating an upstream cause that was never looked at.
None of that is glamorous, and none of it is a single magic supplement. It is the unflashy maintenance that decides whether the result holds.
What this means for the woman in front of me. If your last protocol ended at the clean retest and nothing came after it, that gap is worth naming out loud. The after-care is not optional. It is the part that protects the win you already earned.
Does a positive breath retest mean my SIBO is back?
A positive retest is a signal worth discussing, not proof your SIBO has returned. This is one of the most important things I can hand you, because it can save you from a treatment round you may not need. The breath test is the standard tool, and it is shakier than most people are told.
A breath test measures the gases your gut microbes produce after you drink a sugar solution. The trouble is what those gases actually reflect. A lactulose breath test largely measures how fast things move through you, with sensitivity around 42% (Kashyap 2024).
Lactulose is the sugar used in many of these tests. So a “positive” can sometimes mean fast transit, not a true overgrowth.
What conventional medicine misses here, and what the wellness industry overstates in the other direction, is the same thing. The number is a signal, not a verdict. A leading neurogastroenterology appraisal in 2024 argued the whole breath-test construct has been stretched past what it can support.
What this means for the woman in front of me. Treat a positive retest as one input in a conversation, not as automatic permission for another antibiotic round. Symptoms, history, and pattern matter at least as much as the number.
What I’d do this week
If you take one thing from this, take the framework below. It is an educational map, not a treatment protocol, and it is built to be saved and re-opened before your next appointment. Bring it. Ask the questions in it out loud.
Caveat (always read with the card). A positive breath retest is not proof of relapse. A lactulose breath test largely reflects how fast things move through you, with sensitivity around 42% (Kashyap 2024). Treat a number as a signal, not a verdict. And “natural” does not mean “safe for everyone.” Berberine and oregano oil are contraindicated in pregnancy and lactation, and berberine interacts with several medications.
Red flags that always route to a conventional workup first. Blood in stool, unexplained weight loss, severe pain, iron deficiency without a cause, new GI symptoms over 50, or a family history of GI cancer. So here is your one job this week. Stop asking “which type am I” and start asking “what keeps letting this return.” Then write down the one upstream question from the card that fits your pattern, and bring it to whoever helps you.
The bottom line
I will not tell you SIBO is easy or that one round fixes it. It is a persistent condition, and saying so plainly is the only honest place to start. The relapse you lived through was not your failure. It was an unanswered question about what was keeping the door open.
The good news is that the question has answers. Most of them live upstream of the bacteria, in motility, in your history, and in what happens after the kill rather than during it. What is the one thing you were never told about why yours keeps coming back? That is the conversation worth having next.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Frequently asked questions
How long after SIBO treatment does it usually come back? Recurrence builds over time rather than all at once. Across cohort data, relapse rises to roughly 13% at three months, 28% at six months, and about 44% by nine months after a single antibiotic course. This is why a clean retest right after treatment does not guarantee the result will hold.
Is methane SIBO harder to treat than hydrogen SIBO? Methane-type SIBO, now called IMO, tends to be more stubborn because it is tied to slowed gut transit. The slowdown gives the overgrowth time to re-establish, so addressing motility usually matters more here than chasing the gas. A single antimicrobial agent often underperforms against methane compared with a combination approach.
Can I treat SIBO with herbs instead of antibiotics? In one head-to-head trial, herbal antimicrobials cleared SIBO comparably to rifaximin, with fewer reported side effects. That said, it was a single open-label study, so the evidence is encouraging rather than settled. Berberine and oregano oil are not safe in pregnancy or lactation, and berberine interacts with several medications, so screen carefully first.
Does a positive breath test mean my SIBO came back? Not necessarily. A lactulose breath test largely reflects how fast food moves through you, and its sensitivity sits around 42%. A positive result is a signal worth discussing alongside your symptoms and history, not automatic proof of relapse. Treat the number as one input, not a verdict.
Can past antibiotic use cause SIBO? It is plausible that repeated antimicrobial rounds reshape the gut environment in ways that leave it more vulnerable to future overgrowth. This is an honest tension, not a reason to fear a single necessary course. The concern is endless cycling without a plan for what comes after the kill.
Why does SIBO relapse if the treatment worked? Relapse usually means the upstream driver was never addressed, not that the kill failed. The most commonly missed driver is slowed motility, the muscular wave that sweeps the small intestine clean between meals. When that sweep stays slow, bacteria regrow regardless of how effective the antimicrobial was.
References
1. Gatta, L., & Scarpignato, C. (2017). Systematic review with meta-analysis: rifaximin is effective and safe for the treatment of small intestine bacterial overgrowth. Alimentary Pharmacology & Therapeutics, 45(5), 604-616. https://doi.org/10.1111/apt.13928
2. Talamantes, S., Steiner, F., Spencer, S., Neshatian, L., & Sonu, I. (2024). Intestinal methanogen overgrowth (IMO) is associated with delayed small bowel and colonic transit time on the wireless motility capsule. Digestive Diseases and Sciences, 69(9), 3361-3368. https://doi.org/10.1007/s10620-024-08563-x
3. Chedid, V., Dhalla, S., Clarke, J. O., Roland, B. C., Dunbar, K. B., Koh, J., Justino, E., Tomakin, E., & Mullin, G. E. (2014). Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine, 3(3), 16-24. https://doi.org/10.7453/gahmj.2014.019
4. Kashyap, P. C., et al. (2024). Critical appraisal of the SIBO hypothesis and breath testing: a clinical practice update endorsed by ESNM and ANMS. Neurogastroenterology & Motility. https://doi.org/10.1111/nmo.14817
5. Zhang, Q., Li, H., Chen, C., Li, M., Song, J., Pan, S., Shen, B., & Huang, Y. (2025). Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis. Therapeutic Advances in Gastroenterology, 18, 17562848251399033. https://doi.org/10.1177/17562848251399033
6. Lu, H. (2026). Relationship between small intestinal bacterial overgrowth and irritable bowel syndrome and the efficacy of rifaximin intervention: a systematic review and meta-analysis. Frontiers in Microbiology, 17, 1780567. https://doi.org/10.3389/fmicb.2026.1780567