Rome V Just Changed Your IBS Diagnosis (June 2026)
If you have ever sat across from a doctor, listed every symptom you have lived with for years, and walked out with the words “it’s just IBS,” you already know the feeling this post is about. The relief of a name. The hollow space right behind it, because a name is not an answer. In 2026, the rulebook for that diagnosis changed. The global criteria that define irritable bowel syndrome, called the Rome criteria, were updated to their fifth edition. The word “functional” is being retired. The bar to qualify for IBS came down. More women will now be told they meet the definition.
Here is what I want you to walk away understanding, and it is the one thing neither the dismissive-doctor camp nor the wellness-cure camp will tell you. A better name and a wider net reduce stigma and let more women finally be believed. They do not locate what is driving your symptoms. If you now qualify for IBS, that label is an invitation to keep asking why, not a place to stop looking. Below, I will walk through exactly what changed, what the evidence says, what to ask if you are handed this label, and the red flags that always need a conventional work-up first.
What conventional medicine misses when it renames a diagnosis
Conventional medicine just did something genuinely useful and slightly sleight-of-hand at the same time. It gave a stigmatized condition a more accurate, less dismissive name. What it did not do is add a single test that finds the cause underneath your symptoms. That gap is the whole story.
Let me back up a little bit. For most of its history, IBS sat inside a category called “functional gastrointestinal disorders.” In medicine, “functional” is supposed to mean a problem with how an organ works rather than a visible structural lesion. In the real world, women heard it differently. They heard “we found nothing,” “this is probably stress,” “it might be in your head.” That word did real damage to real people who were not being taken seriously.
The honest center of this whole topic: renaming a disorder reduces the stigma attached to it, but it does not, on its own, identify what is driving any one woman’s symptoms. That is the naturopathic lens on this. The root-cause version of the question is not “what is this called now,” it is “why is my gut doing this, and what under the label is still worth investigating.”
This is where my view parts from both extremes. The dismissive side treats IBS as a wastebasket diagnosis, a polite way to stop looking. The wellness side will read the rename as proof someone finally cracked IBS, then sell you the supplement that supposedly fixes it. Neither is honest. The truth sits in the middle, and it is less satisfying and more useful than either.
What is Rome V and what actually changed in 2026?
Rome V is the 2026 fifth edition of the global criteria doctors use to diagnose IBS and related gut conditions. It minimizes the word “functional,” renames the category “disorders of gut-brain interaction,” re-includes “discomfort” alongside pain, and lowers the symptom-frequency threshold, so more people now meet the definition.
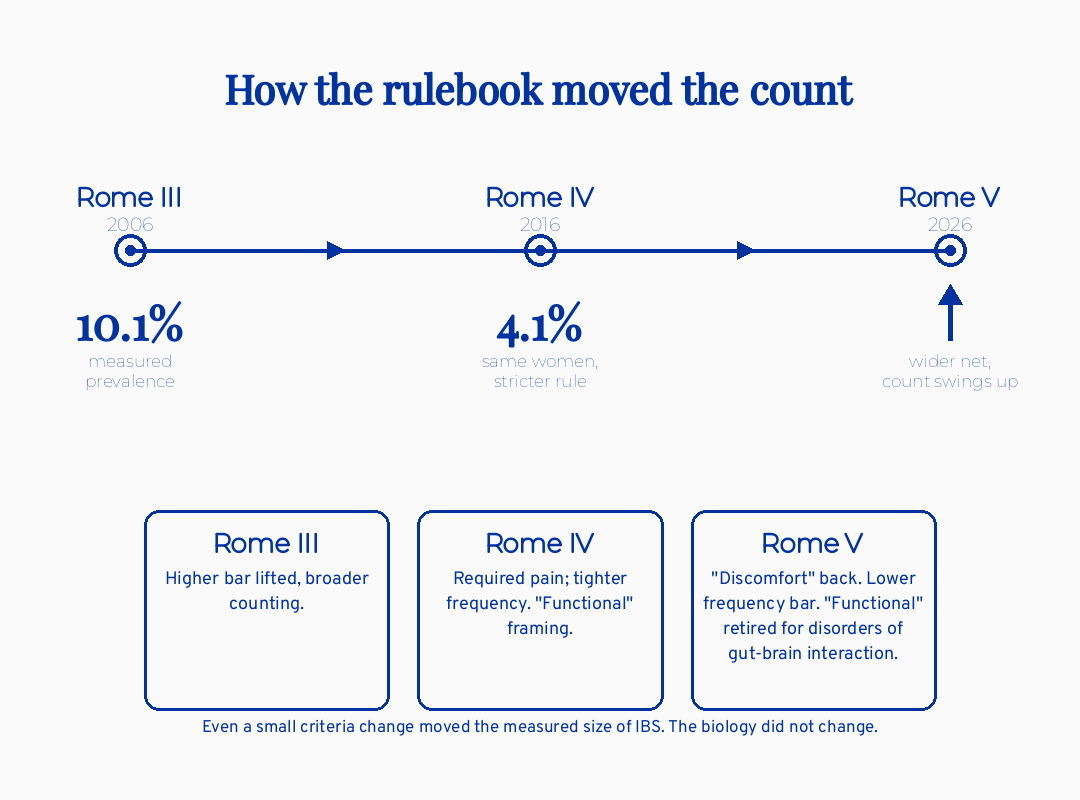
Think of the Rome criteria as the official rulebook for a diagnosis you cannot see on a scan. There is no blood test for IBS. There is no biopsy. So a committee of international gastroenterologists defines, in writing, the exact pattern of symptoms that counts. Rome IV was the 2016 version. Rome V is the 2026 update. When that rulebook changes, the number of people who “have” IBS changes overnight, without anyone’s gut changing at all.
Four shifts matter for you. First, “functional” is being retired in favor of physiologically precise language. “Functional constipation” becomes “chronic constipation.” Second, “discomfort” is back. Rome IV had stripped it out and required pain specifically. Many women describe pressure, fullness, or gnawing unease rather than sharp pain, and the old wording quietly excluded them. Third, the frequency bar came down, so symptoms that happen less often still count. Fourth, the criteria now formally write dietary and behavioral care into the framework rather than treating it as an afterthought.
Bottom line on the change: Rome V is a clearer, kinder label with a wider net. It is not a found cause. The committee added no root-cause test. That is not a criticism. It is just the honest shape of what happened.
Here is the number that makes the slipperiness concrete. Under the old criteria, IBS prevalence fell from 10.1% to 4.1% on one pain-frequency rule (Tornkvist 2025). One rule. The measured size of an entire condition more than halved, not because women got healthier, but because the definition tightened. Rome V loosens that same lever, which is why the count will swing back up.
Why will more women be told they have IBS now?
More women will qualify because Rome V re-added “discomfort” and lowered how often symptoms must occur. IBS is already more common in women than men, with functional gut disorders carrying roughly 1.7 times the odds in women in the largest global survey. A lower bar plus a female-predominant condition means the newly captured group skews heavily toward women.
I want to sit with you on this one, because it cuts two ways and you deserve both edges. If you have spent years being told your gut symptoms were too mild, too vague, or too intermittent to be “real,” this change is on your side. The old criteria were genuinely too strict. Validation work showed it: loosening the pain-frequency rule lifted IBS detection sensitivity from 82% to 90% (AP&T 2024 validation). In plain terms, the stricter definition was missing close to one in ten people a clinician already believed had IBS. Rome V is the field correcting that miss.
That is the relief side. Now the honest other edge.
A wider net also means more women handed a chronic-sounding diagnosis for symptoms that are mild, occasional, or tied to their cycle. IBS symptoms can shift across the menstrual cycle and into perimenopause. A low threshold may scoop up cyclic gut changes and label them a disorder. That is not a reason to dismiss your symptoms. It is a reason to stay curious about what is actually driving them, because “you qualify for IBS” and “we understand your gut” are not the same sentence.
The reframe I want you to hold: being believed is the floor, not the ceiling. A label that finally fits is the start of the real work, not the end of it. This is the same pattern I see across gut conditions, and it is part of why a probiotic alone rarely fixes IBS: the label and the quick fix both skip the question of mechanism.
Does “gut-brain interaction” mean it’s all in my head?
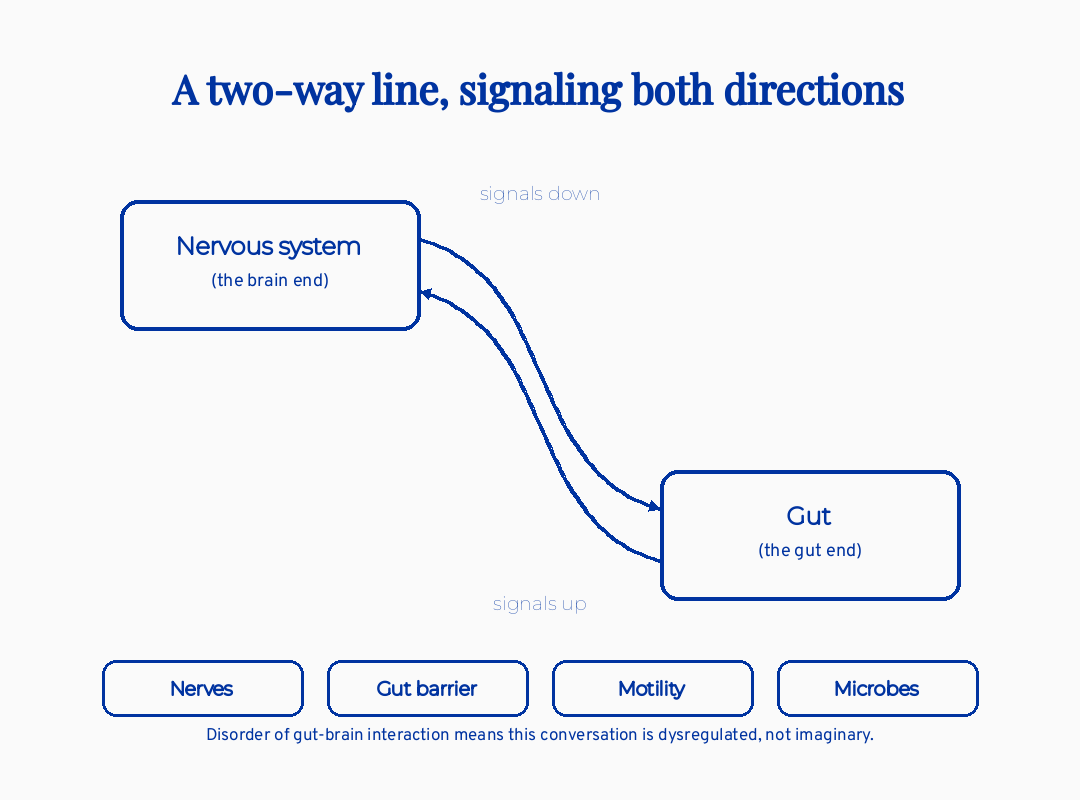
No. “Disorder of gut-brain interaction,” or DGBI, describes real two-way signaling between your gut and your nervous system. It is not a euphemism for psychological. The biology involves nerves, the gut barrier, gut movement, and the microbes living in your intestines, all sending signals in both directions, and that signaling is measurable.
Let me define the term plainly, because the name is doing a lot of work and it is easy to misread. A disorder of gut-brain interaction means the conversation between your gut and your brain is dysregulated. Picture a phone line between two cities that stays open in both directions all day. When the line gets noisy, both ends misfire. Pain signals get amplified. Gut movement speeds up or stalls. The brain reads ordinary gut sensations as alarming.
One piece of that biology deserves its own plain-language definition. Visceral hypersensitivity means the nerves in your gut wall are turned up too high, so a normal amount of gas or stretch registers as real pain. It is not imagined pain. It is a genuine signaling problem in genuine nerves. Mechanistic reviews tie DGBI to visceral hypersensitivity, altered gut movement, low-grade immune activation, and shifts in the microbiome, with stress acting as one input among several rather than the whole explanation.
Here is where the rename can backfire if you are not careful. “Gut-brain” gets collapsed into “just stress,” which revives the exact dismissal Rome V was trying to bury. Stress is one contributor. So is a prior gut infection. So is how your gut moves food through. The biology is multifactorial, which is precisely why no single rename produces a single test, and why no single supplement can claim to fix it. If you want the deeper version of how hormones layer onto this, I have written about how perimenopause shifts gut symptoms through the estrogen-gut axis.
If the label has no test, is an IBS diagnosis even safe to trust?
Yes, a positive IBS diagnosis made with limited testing holds up over time. In a roughly four-year follow-up of patients diagnosed this way, the rate of later discovering a missed organic disease was only about 1%. So “they just called it IBS” is not the same as “they failed to rule out something serious,” as long as the basics were checked.
I want to name the fear directly, because I have seen it in cases I have reviewed and in the questions women send me. The fear is that “IBS” is what doctors say when they have given up, and that something dangerous is hiding behind it. That fear is reasonable. It is also, for the most part, not what the data shows.
A positive IBS diagnosis missed organic disease in about 1% of patients over four years (CGH 2023). That is genuinely reassuring. It means the diagnostic strategy of recognizing the symptom pattern, checking for alarm features, and running limited tests is safe and durable. The problem with the old Rome IV criteria was never that they were dangerous. The problem was sensitivity. They missed real patients who had IBS, not that they mislabeled sick people as healthy.
So both things are true at once, and I am not going to smooth that over for you. The diagnosis is safe and the old net was too narrow. The new net is wider and risks labeling milder symptoms as a disorder. Holding both is the honest position. The label being trustworthy does not mean the inquiry should stop.
The clinical bottom line: a careful IBS diagnosis is safe to trust as a starting point. Safe to trust does not mean finished.
What is the root cause of IBS if Rome V didn’t find one?
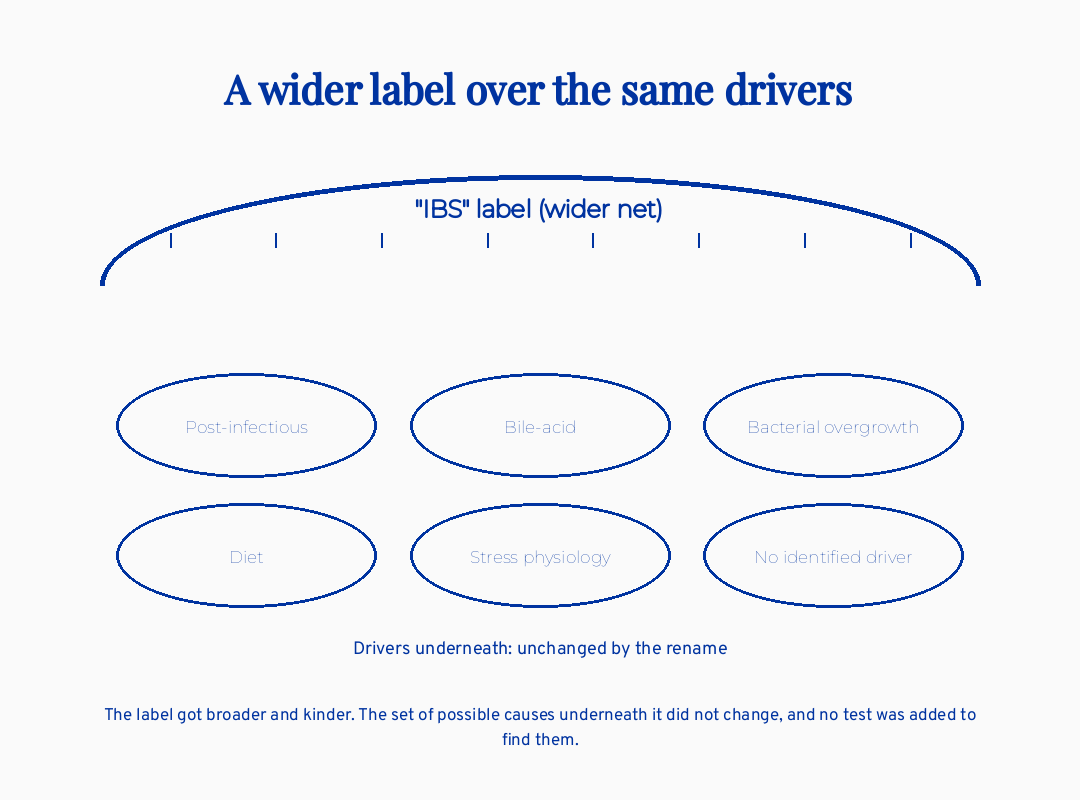
There is no single root cause of IBS, and that is the honest answer the rename does not change. Some cases trace to a prior gut infection, some to bile-acid issues, some to bacterial overgrowth, some to diet, some to stress physiology, and some have no identifiable driver on standard testing. The label sits on top of many different stories.
This is the part where I have to be a real clinician with you rather than a comforting one. Post-infectious IBS is a recognized pattern worth naming. It means IBS symptoms that begin after a gut infection, a bad stomach bug, or sometimes a course of antibiotics, when the gut never fully reset afterward. If your symptoms started after a discrete event like that, it is a thread worth pulling, because it points toward a mechanism rather than a mystery.
But here is the truth I hold for the women I work with, and it is my locked clinical position, word for word: “There may be a deeper issue going on, and I’ll use all the available research and testing to find out, but there is the possibility of not being able to find the root cause due to limits of current research. We will do the best we can to manage symptoms without being overwhelmed.”
I say it that way on purpose. It refuses the false promise of a guaranteed root cause, and it refuses the false comfort of “it’s just IBS, learn to live with it.” The real work is somewhere in between: investigate seriously, name uncertainty honestly, and manage symptoms without letting the search consume your life.
One mechanism the wellness world loves to crown as the answer is “leaky gut.” Intestinal permeability is real and is one mechanism in some patients. It is not a proven single cause of IBS, and naming it does not earn anyone the right to sell you a fix. Real but overused is the right frame for most single-cause IBS explanations you will see online.
What I’d do this week
If I were sitting with you after a Rome V IBS diagnosis, I would not hand you a supplement. I would hand you better questions. Save the card below for your next appointment. You can also save it as a standalone resource at blueyarrow.org/rome-v-ibs-reclassification.
This is a conversation tool, not a treatment plan, and not a substitute for your own clinician’s judgment.
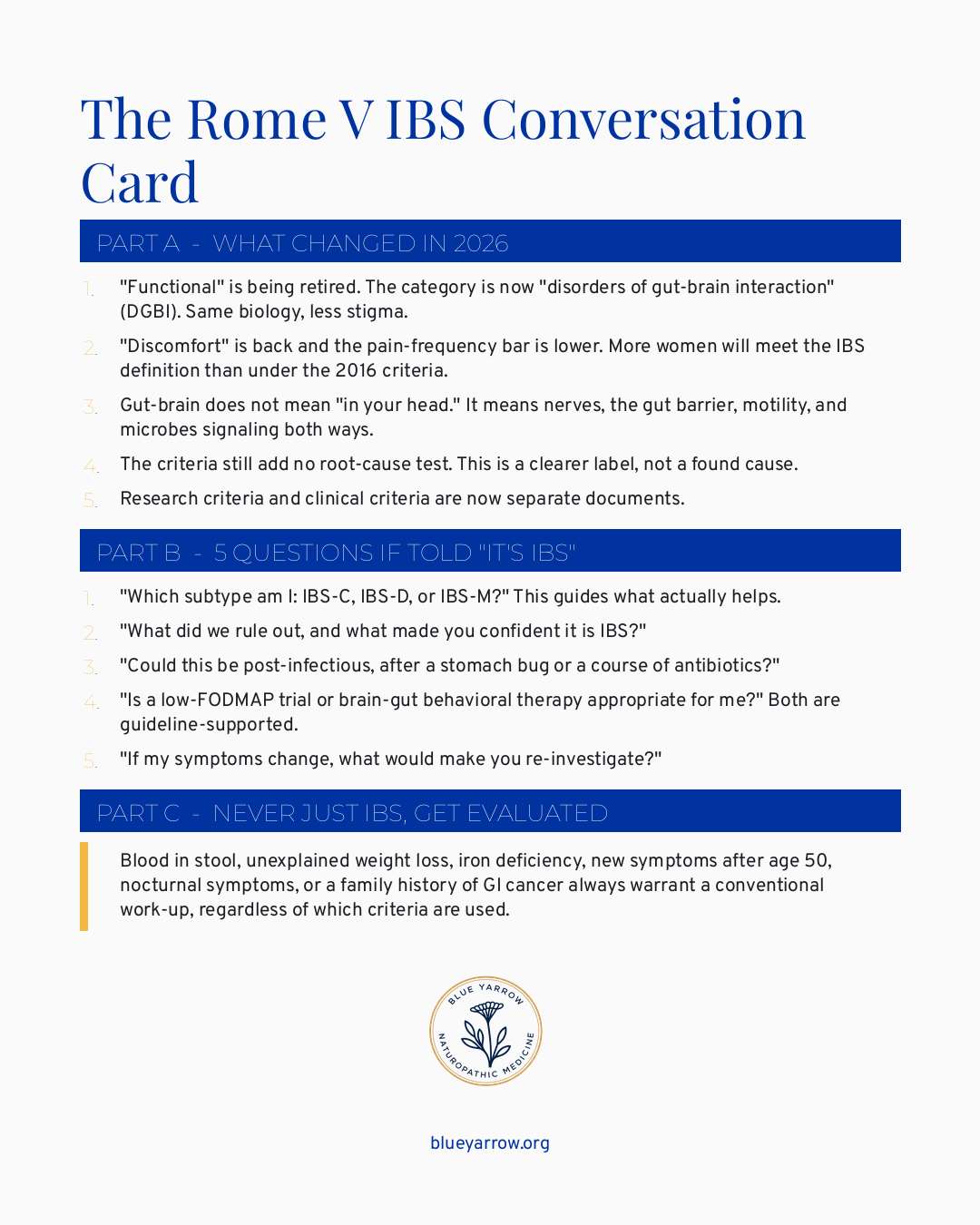
Two of those terms deserve a plain definition before you use the card. A low-FODMAP trial is a short, structured reduction of certain fermentable carbohydrates that feed gut bacteria and produce gas, run as a test rather than a forever diet. Brain-gut behavioral therapy is a set of evidence-based talk and relaxation techniques that quiet the overactive gut-brain signaling, not a suggestion that your symptoms are imaginary. Both sit in the major guidelines as legitimate first-line options.
The save-worthy takeaway: walk in with your subtype question, your rule-out question, and your re-investigate question already written down. That alone changes the appointment.
A note on the two women I keep thinking about
In cases I have reviewed, two patterns show up again and again, and they are almost mirror images.
The first is a woman in her late thirties whose symptoms started after a brutal bout of food poisoning on a trip. For three years she was told it was stress. Under the strict 2016 criteria, her intermittent discomfort technically did not clear the pain-frequency bar, so she kept failing to “officially” qualify, which made her feel like a fraud in her own body. Her story is exactly the kind Rome V is built to catch. The newer criteria would have believed her sooner. That is the win, and it is a real one.
The second is a woman in her early forties whose gut symptoms track tightly with her cycle and have grown louder as perimenopause arrived. Under the lower Rome V threshold, she now cleanly qualifies for IBS. The risk for her is the opposite one. A confident label could close the door on the cyclic, hormonal driver sitting right underneath it. For her, “you have IBS” is the moment to ask more questions, not fewer.
Same diagnosis. Opposite lessons. That is why I refuse to give you a one-line verdict on whether the Rome V change is good or bad. For the first woman it is overdue justice. For the second it is a door that could close too early. The label is a tool. What you do with it is the medicine.
Frequently asked questions
What is the difference between Rome IV and Rome V for IBS? Rome IV (2016) required pain and used a stricter frequency threshold, which excluded many real patients. Rome V (2026) re-includes “discomfort,” lowers the frequency bar, and retires “functional” in favor of “disorder of gut-brain interaction.” The net effect is a wider, less stigmatizing definition that captures more women.
Does the Rome V change mean doctors found the cause of IBS? No. Rome V is a renaming and a recalibration of criteria, not a discovery. The committee added no biomarker and no root-cause test. It reduces stigma and broadens who qualifies, but it does not identify what is driving any individual person’s symptoms, which is why the inquiry should continue after diagnosis.
Is IBS a real diagnosis or just a label doctors use to stop looking? It is real. A positive IBS diagnosis made with limited testing is durable, with only about a 1% rate of later finding a missed organic disease over four years. The biology behind it, involving nerves, gut movement, and the microbiome, is measurable. It is a real condition, not a verbal shrug.
Does “disorder of gut-brain interaction” mean my IBS is caused by anxiety? No. Gut-brain interaction means two-way signaling between gut and nervous system, and stress is one contributor among several, including prior infection, altered motility, immune activation, and microbiome shifts. Collapsing “gut-brain” into “anxiety” revives the exact dismissal the new name was designed to reduce.
Will more people be diagnosed with IBS under Rome V? Almost certainly. Under prior criteria, measured IBS prevalence dropped from about 10% to 4% on one frequency rule alone. Rome V loosens that lever, so the count will rise. Because IBS is female-predominant, the newly captured group will skew toward women.
What symptoms mean I should not accept an IBS label without more testing? Blood in stool, unexplained weight loss, iron deficiency, new symptoms starting after age 50, symptoms that wake you at night, or a family history of gastrointestinal cancer all warrant a conventional work-up regardless of which criteria are used. These alarm features should never be folded into an IBS diagnosis without evaluation.
The one question I want to leave you with
If a doctor told you “it’s IBS” tomorrow, would you know which of the five questions on that card to ask first? Pick the one that matters most for your own story, write it down, and bring it. Being believed is the floor. Staying curious is the medicine.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Sperber, A. D., Bangdiwala, S. I., Drossman, D. A., et al. (2020). Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome Foundation Global Study. Gastroenterology, 160(1), 99-114. https://doi.org/10.1053/j.gastro.2020.04.014
2. Tornkvist, N., Palsson, O. S., Hreinsson, J., Sperber, A. D., Bangdiwala, S. I., Tornblom, H., & Simren, M. (2025). Global prevalence, characterization and impact of functional bowel disorders. American Journal of Gastroenterology. https://doi.org/10.14309/ajg.0000000000003782
3. Validating simple modifications to the Rome IV criteria for IBS in secondary care. (2024). Alimentary Pharmacology & Therapeutics. PMID 39466700. https://pubmed.ncbi.nlm.nih.gov/39466700/
4. Assessing diagnostic performance of modifications to the Rome IV criteria for IBS. (2024). Clinical Gastroenterology and Hepatology. PMID 38423348. https://pubmed.ncbi.nlm.nih.gov/38423348/
5. A diagnosis of IBS using Rome IV criteria and limited investigations is durable in secondary care. (2023). Clinical Gastroenterology and Hepatology. https://www.cghjournal.org/article/S1542-3565(23)00444-5/fulltext
6. Kraimi, N., Ross, T., Pujo, J., & De Palma, G. (2024). The gut microbiome in disorders of gut-brain interaction. Gut Microbes, 16(1), 2360233. https://doi.org/10.1080/19490976.2024.2360233
7. Leigh, S.-J., Uhlig, F., Wilmes, L., et al. (2023). The impact of acute and chronic stress on gastrointestinal physiology and function: A microbiota-gut-brain axis perspective. The Journal of Physiology, 601(20), 4491-4538. https://doi.org/10.1113/JP281951
8. Melchior, C., Hammer, H., Bor, S., et al. (2025). European consensus on functional bloating and abdominal distension: An ESNM/UEG recommendation for clinical management. United European Gastroenterology Journal, 13(9), 1613-1651. https://doi.org/10.1002/ueg2.70098
9. American College of Gastroenterology. (2021). ACG clinical guideline: Management of irritable bowel syndrome. American Journal of Gastroenterology.
10. Rome Foundation. (2026). Rome V: A global framework for disorders of gut-brain interaction. theromefoundation.org