Your Gut Shifts in Perimenopause. Your Heart Listens.
If you’ve noticed your gut and your heart both feel different lately, and your labs came back fine, you are not imagining it. I hear the same three sentences from women in their early forties over and over. “My labs are normal but I know something is off.” “No one told me my gut would change like this.” “My heart races out of nowhere and I’m only 43.” You are not falling apart, and you are not too young. Something real is happening, and most of the time no one connects the pieces for you.
Here is the piece almost no one is saying out loud yet. As estrogen starts to drop in perimenopause, your gut changes in measurable ways, and researchers are now asking whether that gut change is one of the threads tying this transition to heart risk. I want to walk you through what the science actually supports, what it doesn’t yet, and the food-first moves that have real human data behind them. By the end you’ll know what to ask for and what to ignore on the supplement shelf. Let me back up and explain it the way I’d explain it to a friend who just got told she’s fine.
The short version: the gut shift after estrogen declines is real and human-supported. The heart half of the story is a serious, named hypothesis, but the direct cardiovascular evidence so far comes from animal studies. So the proven lever is food, not a probiotic promise.
What is the estrobolome, and why does it matter in perimenopause?
The estrobolome is the collection of gut bacteria that recycle and regulate the estrogen circulating in your body. That recycling step is real, it is human-supported, and it matters most exactly when estrogen starts to fall.
Here’s the mechanism in plain language. Your liver tags used estrogen with a molecular flag so your body can clear it out. Certain gut bacteria carry an enzyme called beta-glucuronidase (an enzyme that snips that flag back off), which frees the estrogen to be reabsorbed instead of excreted. That loop, the deconjugation-and-reabsorption cycle, is what researchers call the estrobolome at work (Baker 2017; Hu 2023). When the bacteria carrying that enzyme shift, the amount of estrogen your body holds onto can shift too. This part of the story has solid review-level data behind it. It is not the speculative part.
What this means for the woman in front of me: the gut is not a side character in your hormone story. It is part of the machinery. When you feel like your digestion and your cycle started misbehaving in the same season, that is not a coincidence you invented.
The estrobolome is the human-supported anchor of this whole topic: gut bacteria genuinely participate in how much estrogen stays in circulation.
Why is my gut suddenly changing in my forties?
As estrogen declines through perimenopause, the gut microbiome tends to lose diversity and shift, and that is one reason gut symptoms cluster so heavily in this transition. The data here is strong, not speculative.
A woman I’ll call Maya, 39, told me she’d never had a sensitive stomach in her life and then, almost overnight, bloating became her default state. She’d been told she was too young for perimenopause. She wasn’t. Reviews of the menopausal transition consistently show reduced microbial diversity and a shift toward a less estrogen-friendly profile as estrogen falls (Peters 2022; Lim 2026). That tracks with how common these symptoms are. A study presented at The Menopause Society in 2025 found that 94 percent of women report digestive symptoms in perimenopause and 77 percent report bloating. So when you say “no one told me my gut would change like this,” the honest answer is that the science agrees with your body, even if your last appointment didn’t.
Estrogen also helps maintain the gut barrier, the single-cell lining that decides what gets into your bloodstream and what stays in your gut. Think of it like the grout between bathroom tiles. When it holds, the wall does its job. When estrogen drops, that barrier can loosen, a pattern often called increased intestinal permeability or “leaky gut” (Meng 2024; Zhu 2026). I want to be precise here, because this is where the human evidence gets thinner and the animal evidence gets stronger, and I’ll come back to that distinction in a moment.
What this means for the woman in front of me: your gut symptoms are early information, not a character flaw, and they showed up on schedule with a hormonal change you can’t see on a standard panel.
As estrogen declines, gut diversity drops and the barrier can loosen. That shift is well-described in humans and explains why bloating and digestive changes are nearly universal in perimenopause.
Is my gut really connected to my heart in perimenopause?
This is the part to handle with care. Researchers are now mapping an estrogen-gut-vascular axis, the idea that the gut shift after estrogen loss may be one mechanism linking perimenopause to rising heart risk. In humans this is still an emerging hypothesis, and the direct heart evidence so far is from animal studies.
Let me lay out the proposed chain honestly. The framework, published as a 2026 review, runs like this: estrogen falls, the gut barrier loosens, beneficial short-chain fatty acids (SCFAs, fuel your gut lining makes from fiber) decline, pro-inflammatory metabolites and bacterial fragments like LPS (lipopolysaccharide, a piece of bacterial outer wall that triggers inflammation when it leaks into the blood) rise, and that low-grade inflammation nudges atherosclerosis along (atherosclerosis is the slow buildup of plaque in artery walls) (Zhu 2026). It is a coherent, named story. But here is where I refuse to overstate it: every demonstration that fixing the gut actually slows plaque comes from ovariectomized mice, where fecal transplant and estrogen reversed the damage (Meng 2024; Meng 2021). That is a strong animal signal. It is not a human outcome. Emerging hypothesis, the direct heart evidence so far is from animal studies.
What is rock solid, completely separate from the gut question, is the timing. Perimenopausal women are roughly twice as likely as cycling women to score low on cardiovascular health (AHA 2026). The American Heart Association is now calling this transition a window of opportunity for heart attention. So the heart deserves your attention in your forties regardless of whether the gut bridge ever gets proven in humans.
A second woman I’ll call Renee, 44, came across one of these reviews and arrived convinced her palpitations were “leaky gut hitting her heart.” I understand the appeal of a clean single cause. But the careful read is that her heart deserved a real cardiovascular look on its own merits, and the gut was a reasonable thing to support with food, not a diagnosis to pin the palpitations on.
What this means for the woman in front of me: take the heart window seriously now, and treat the gut-heart bridge as a promising idea worth understanding, not a proven pipeline you can fix with a capsule.
The gut-to-heart link is a real, published hypothesis, but the causal heart evidence is animal-level. The perimenopause heart window itself is human-proven and worth your attention now.
Why are my labs normal when my body clearly isn’t?
Because perimenopause has no reliable single biomarker. FSH and estrogen swing wildly week to week, so one blood draw can look textbook while you feel like a stranger in your own body. A normal panel is a snapshot of one moment, not proof you’re fine.
This is the gap that makes so many women feel gaslit. Your symptoms are real evidence. They are simply evidence a single hormone snapshot is not built to capture. In cases I’ve reviewed, the women who feel most dismissed are often the ones whose labs are technically unremarkable, which is precisely why I’d rather look at the pattern across symptoms, cycle changes, gut shifts, and cardiovascular risk markers together than chase one number on one day.
Here is the reframe I’d want you to hold. Perimenopause is not a hormone deficiency you can read off a single test. It is a hormone variability event, and variability is hard to photograph. The standard workup is built to rule out disease, not to map a transition. Both things can be true at once: your labs can be normal and your experience can be completely valid.
What this means for the woman in front of me: if you’ve been handed a normal lab and a shrug, that does not close the case. It means the test answered a narrow question and your fuller story is still worth telling to someone willing to listen.
Perimenopause has no single reliable biomarker, so normal labs and real symptoms coexist constantly. Your symptoms are data, not drama.
Will a probiotic fix my estrogen and protect my heart?
The honest answer is no, not in the way the marketing implies. There is no human outcome trial showing any gut product balances perimenopausal hormones or protects the heart, and the one human trial touching estrogen is a single, exploratory, industry-funded study using a surrogate marker.
I want to be fair to the science that does exist, because some of it is genuinely interesting. One beta-glucuronidase-active probiotic maintained serum estrogen over 12 weeks in healthy peri- and postmenopausal women, while the placebo group declined (Honda 2024). That is a real finding. It is also a single study, funded by the company that makes the strain, measuring a blood level rather than how anyone felt or any heart outcome. Early studies look promising, but this one is not settled, and one trial measuring a surrogate is not a reason to spend money on a promise.
The strongest counterweight is the one the supplement aisle never mentions. A 1,000-person study found no estrobolome signal in an estrogen-driven condition, a caution against gut-fixes-hormones claims (Perez-Prieto 2024). When researchers tested the estrobolome at real human scale, in a condition where you’d expect it to show up, it produced a clean null, even after they excluded older women in a sensitivity check. That doesn’t erase the recycling mechanism. It does mean the leap from “the mechanism is real” to “so this product fixes it” is a leap the human data has not made.
And there’s a humbling fact underneath all of it: no validated “ideal” estrobolome exists. Profiles vary by geography and ethnicity, so chasing a perfect gut profile is chasing a target no one has actually located (Lim 2026; Peters 2022). What I share with people who ask me about estrobolome products is this: the mechanism is real, the outcome promise is not earned, and the gut-to-heart claim rests on animal data. Emerging hypothesis, the direct heart evidence so far is from animal studies.
What this means for the woman in front of me: save your money and your hope for what actually moves the needle, and treat any product promising to “balance your hormones and protect your heart” as marketing running ahead of the evidence.
No gut product has human outcome data for hormones or heart. The recycling mechanism is real; the fix-it promise is not earned.
What about HRT and the estrogen paradox?
HRT is genuinely worth discussing for some women, and it is individualized. It is not a universal answer, and the cardiovascular picture is more complicated than either side of the internet makes it sound.
Here is the paradox in plain terms. Estrogen looks cardioprotective in observational data, yet hormone therapy trials have been messier than that simple story predicts. One of the reasons researchers are interested in the gut at all is the possibility that it sits somewhere in the middle of that puzzle, an intermediary that might help explain why restoring estrogen isn’t automatically and cleanly heart-protective. That is part of why the gut-vascular work exists, and it is also a reason not to assume any estrogen-restoring move is guaranteed to help your arteries. Emerging hypothesis, the direct heart evidence so far is from animal studies.
What I won’t do here is tell you a dose, a route, or a specific compound. That is an individual decision between you and a prescriber who knows your full risk picture, including your cardiovascular and breast history. What I will say is that HRT belongs on the table as a conversation for many women in this window, framed as your personal risk-benefit, not as a yes-or-no for everyone.
What this means for the woman in front of me: bring HRT up as a real question, expect an individualized answer, and be skeptical of anyone, in either direction, who gives you an absolute.
HRT is individualized, not universal. The estrogen paradox is exactly why no one should promise that restoring estrogen automatically protects your heart.
What I’d do this week
If you take one thing from this, let it be food first, supplements last, and no outcome promises. Here is the card I’d want you to screenshot and bring to your next appointment or your next trip down the supplement aisle.
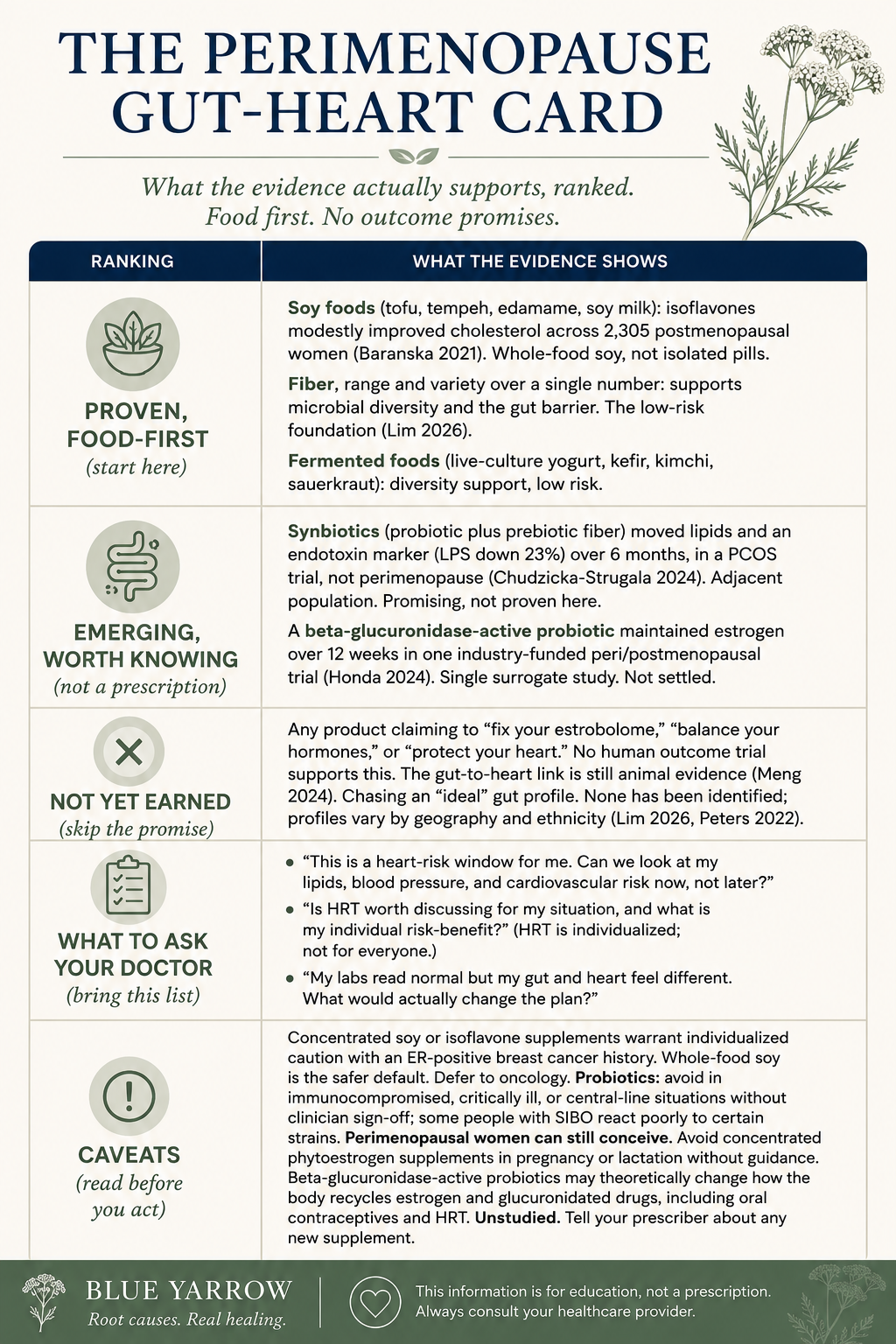
Why food carries the weight here is simple. Soy isoflavones modestly lowered total cholesterol across 2,305 postmenopausal women versus placebo (Baranska 2021 meta-analysis). That is human, pooled-trial evidence in roughly the right population, which is exactly what the supplement claims lack. Start with the things that have data and almost no downside.
The bottom line on your gut, your hormones, and your heart
Three things are true at once, and holding all three is the honest position. Your gut genuinely shifts as estrogen declines, and that shift is human-supported. The heart deserves real attention in this window, because perimenopausal women are roughly twice as likely as cycling women to score low on cardiovascular health (AHA 2026). And the bridge between the two, the gut-to-heart story, is a credible, named hypothesis whose direct cardiovascular evidence is still from animal studies.
So the move is not to chase a perfect estrobolome or a probiotic that promises your heart. The move is to eat for your gut and your lipids with food that has real data, take the heart window seriously now, and bring the right questions to someone willing to look at the whole pattern instead of one normal lab. You felt something change. You were right to.
What is the one symptom in this transition you most wish someone had connected for you?
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Frequently asked questions
Does the gut affect estrogen in perimenopause? Yes. Gut bacteria carry an enzyme, beta-glucuronidase, that recycles estrogen back into circulation rather than letting it be excreted. This estrobolome activity is human-supported. As estrogen declines, gut diversity tends to drop, which is one reason digestive symptoms cluster so heavily during the perimenopausal transition.
Can a probiotic balance my hormones or protect my heart? No gut product has human outcome data showing it balances perimenopausal hormones or protects the heart. One small, industry-funded trial maintained serum estrogen on a single strain over 12 weeks, but that is a surrogate marker, not a symptom or heart result, and it has not been replicated. Treat such promises as marketing.
Is the gut-heart connection in menopause proven? It is a serious, named hypothesis, not proven in humans. Researchers describe an estrogen-gut-vascular axis, but every demonstration that fixing the gut slows plaque comes from animal studies. The perimenopause heart-risk window itself is human-proven, so the heart deserves attention now regardless of the gut question.
Why are my labs normal if I feel terrible in perimenopause? Perimenopause has no reliable single biomarker. FSH and estrogen swing wildly week to week, so one blood draw can look normal while your body clearly says otherwise. Your symptoms are real data that a single hormone snapshot is not designed to capture, which is why pattern matters more than one number.
Does soy help cholesterol after menopause? Yes, modestly. A meta-analysis of 2,305 postmenopausal women found soy isoflavones lowered total cholesterol and slightly raised HDL versus placebo. Whole-food soy like tofu, tempeh, and edamame is the safer default. Concentrated isoflavone supplements warrant individualized caution with an ER-positive breast cancer history.
Should I take HRT for heart health in perimenopause? HRT is individualized and not a universal answer. Estrogen looks cardioprotective in observational data, yet trials are messier, which is why no one should promise it automatically protects your heart. Discuss your personal risk-benefit, including cardiovascular and breast history, with a prescriber. It is worth the conversation for many women, not all.
References
1. Baker, J. M., Al-Nakkash, L., & Herbst-Kralovetz, M. M. (2017). Estrogen-gut microbiome axis: Physiological and clinical implications. Maturitas, 103, 45-53. https://doi.org/10.1016/j.maturitas.2017.06.025
2. Peters, B. A., Santoro, N., Kaplan, R. C., & Qi, Q. (2022). Spotlight on the gut microbiome in menopause: Current insights. International Journal of Women’s Health, 14, 1059-1072. https://doi.org/10.2147/IJWH.S340491
3. Hu, S., Ding, Q., Zhang, W., Kang, M., Ma, J., & Zhao, L. (2023). Gut microbial beta-glucuronidase: A vital regulator in female estrogen metabolism. Gut Microbes, 15(1), 2236749. https://doi.org/10.1080/19490976.2023.2236749
4. Perez-Prieto, I., Vargas, E., Salas-Espejo, E., Lull, K., … Altmae, S. (2024). Gut microbiome in endometriosis: A cohort study on 1000 individuals. BMC Medicine, 22(1), 294. https://doi.org/10.1186/s12916-024-03503-y
5. Lim, M. J. S., Parlindungan, E., See, E., Gan, C. H., Yap, R., & Yong, G. J. M. (2026). Diet, the gut microbiome, and estrogen physiology: A review in menopausal health and interventions. Nutrients, 18(7), 1052. https://doi.org/10.3390/nu18071052
6. Zhu, Y., & Li, Y. (2026). Gut microbiota in perimenopausal atherosclerosis: The estrogen-gut-vascular axis and personalized cardiovascular prevention. Frontiers in Endocrinology, 17, 1815352. https://doi.org/10.3389/fendo.2026.1815352
7. Meng, Q., Zhang, S., Zhang, C., Liu, B., … Bian, H. (2024). Disordered gut microbiota in postmenopausal stage amplifies intestinal tight junction damage to accelerate atherosclerosis. Beneficial Microbes, 16(1), 67-89. https://doi.org/10.1163/18762891-bja00036
8. Meng, Q., Ma, M., Zhang, W., Bi, Y., … Bian, H. (2021). The gut microbiota during the progression of atherosclerosis in the perimenopausal period shows specific compositional changes and significant correlations with circulating lipid metabolites. Gut Microbes, 13(1), 1-27. https://doi.org/10.1080/19490976.2021.1880220
9. Honda, S., Tominaga, Y., Espadaler-Mazo, J., Huedo, P., Aguilo, M., Perez, M., Ueda, T., & Sawashita, J. (2024). Supplementation with a probiotic formula having beta-glucuronidase activity modulates serum estrogen levels in healthy peri- and postmenopausal women. Journal of Medicinal Food, 27(8), 720-727. https://doi.org/10.1089/jmf.2023.k.0320
10. Chudzicka-Strugala, I., Kubiak, A., Banaszewska, B., Wysocka, E., … Duleba, A. J. (2024). Six-month randomized, placebo controlled trial of synbiotic supplementation in women with polycystic ovary syndrome undergoing lifestyle modifications. Archives of Gynecology and Obstetrics, 311(2), 499-506. https://doi.org/10.1007/s00404-024-07833-3
11. Baranska, A., Blaszczuk, A., Kanadys, W., Baczewska, B., Jedrych, M., Wawryk-Gawda, E., & Polz-Dacewicz, M. (2021). Effects of soy protein containing isoflavones and isoflavone extract on plasma lipid profile in postmenopausal women: Systematic review and meta-analysis of RCTs. Nutrients, 13(8), 2531. https://doi.org/10.3390/nu13082531
12. American Heart Association. (2026). Perimenopause and cardiovascular health: Newsroom statement and Journal of the American Heart Association analysis of nationwide US data.