The Pill Didn’t Break Your Hormones. It Hid the Question.
Maybe you stopped the pill and now you are lying awake at night, watching your skin break out or your period go missing. Maybe you are quietly wondering “will I ever feel normal again.” I want you to know two things. The fear is reasonable. The symptoms are real. Here is the part almost nobody says plainly. For most women, the pill did not break your hormones. It hid a question your body had been asking all along. I am Dr. Shad Abdulla, ND, a naturopathic doctor who reads the actual studies. Below I will give you the timeline, the red-flag rule, and an honest look at which herbs actually fit which woman.
Is “post-pill syndrome” even a real thing?
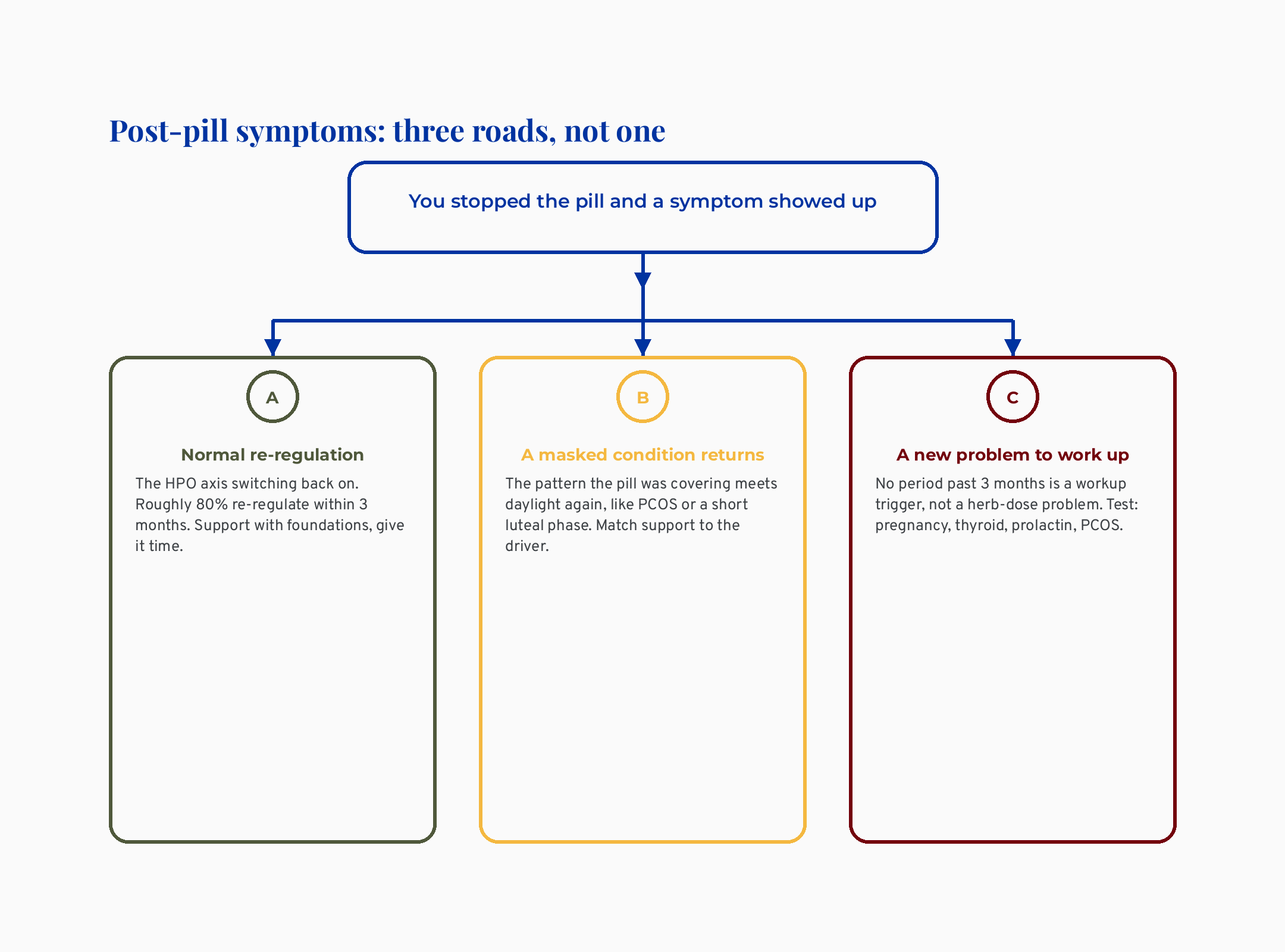
Here is the honest answer up front. “Post-pill syndrome” is not a formal medical diagnosis, but the symptoms women report after stopping the pill are real. They usually fall into one of two buckets: temporary re-regulation, or the return of a pattern the pill was covering up. Naming it that way is not me dismissing you. It is the opposite.
Let me back up a little bit. The term “post-OC syndrome,” meaning post oral-contraceptive syndrome, was coined inside naturopathic writing, not conventional medicine. Conventional bodies do not recognize it as a distinct disease, and they treat the underlying condition instead.
The naturopathic canon does treat it as a real clinical focus worth a plan. Both can be true at once. The symptom cluster is real, AND it is not one tidy disease with one tidy cause.
There is a reason this distinction matters so much. When a label says “syndrome,” it can quietly tell you the problem is one mysterious thing that happened to you. When you understand it as either re-regulation or an unmasked pattern, you get a map instead of a mystery. A map is something you can act on.
What this means for the woman reading this: you are not crazy, and you are not broken. You are meeting your real cycle, sometimes for the first time since you were a teenager.
How long until my period comes back after stopping the pill?
For most women, the period returns within about three months, and the body’s own hormone signaling switches back on during that window. The pill works by switching the HPO axis off, meaning the hypothalamic-pituitary-ovarian axis, the brain-to-ovary signaling loop that runs your cycle. When you stop, that loop wakes back up. It is re-regulation, not repair.
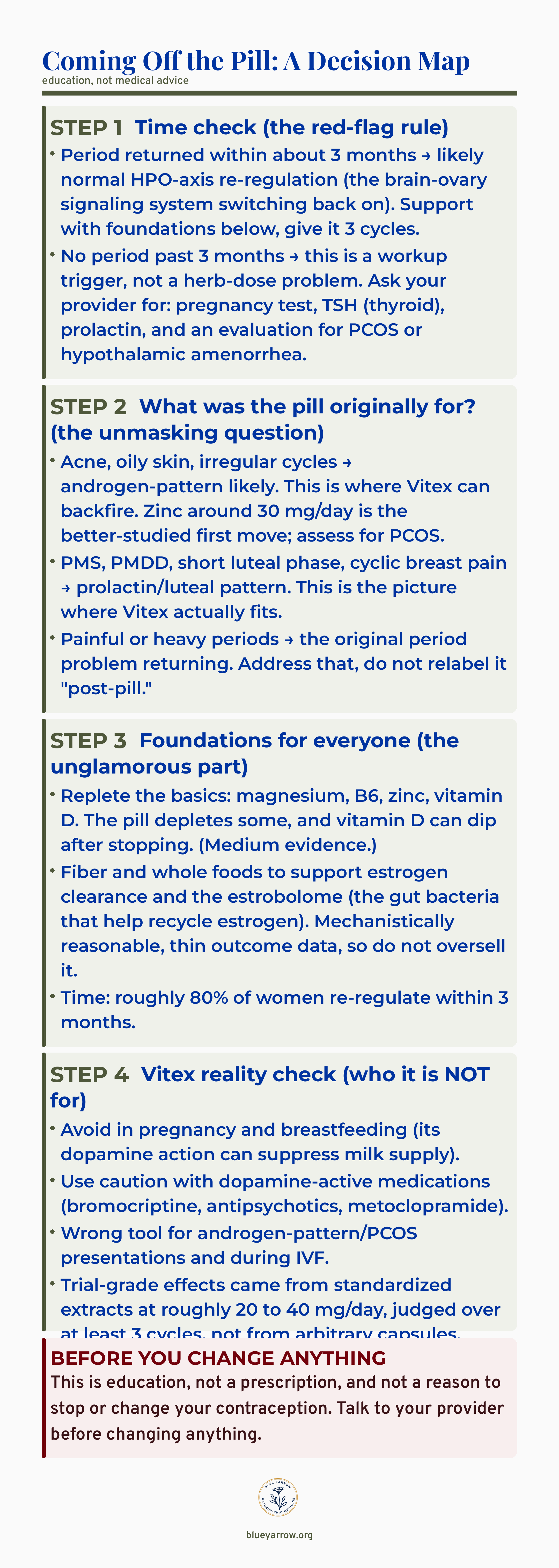
Three months is the line I want you to hold onto. Roughly 80% of women re-regulate inside that window. That is why the unglamorous answer is often time plus a few basics, not a cabinet full of supplements.
This is where I have to be the calm voice. If your period has not returned three months after stopping the pill, get a workup, not another herb. A missing period past three months is a signal to test, not to dose.
For the woman in front of me, the practical takeaway is simple. Mark your calendar from the day you stopped, and give it three cycles before you judge anything.
Did the pill damage my fertility?
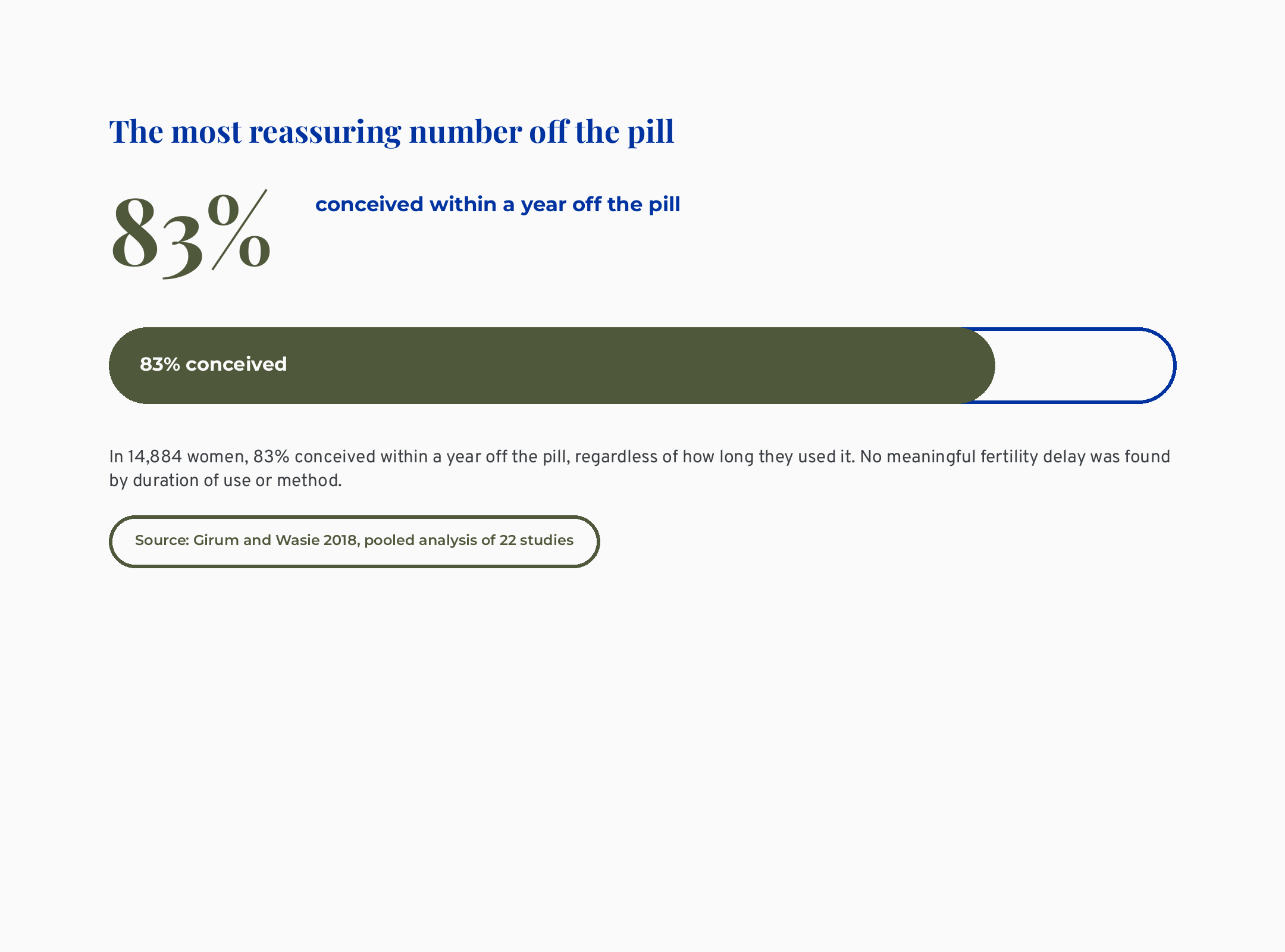
No, and this is the most reassuring number in the whole topic. In 14,884 women, 83% conceived within a year off the pill, regardless of how long they used it (Girum 2018). The evidence here is strong, drawn from a large pooled analysis of 22 studies. It found no meaningful fertility delay by how long you were on it or which method you used.
I know the “I was on it for ten years and now I am terrified” fear is loud. The data does not support lasting fertility damage from the pill itself. When fertility does turn out to be harder, the usual culprit is an unmasked condition like PCOS, meaning polycystic ovary syndrome. Another is hypothalamic amenorrhea, meaning a missing period driven by the brain dialing down the cycle under stress, low body weight, or heavy training.
Here is the naturopathic lens on this. The root-cause version of the question is not “did the pill hurt me,” it is “what was my body already doing that the pill quieted.” That is the more useful question, and it is the one that actually leads somewhere. It also takes the fear and points it at something you can actually investigate.
I want to be fair to the worry, though, because it is not irrational. Many women were put on the pill as teenagers, sometimes before their natural cycle had even settled, so they never got to see their baseline. When that baseline finally shows up at 32, it can look like damage when it is really just information that was hidden for fifteen years.
What this means for you: reassurance is the honest default. If conceiving takes longer than expected, that is a reason to look at the underlying pattern, not to blame the years on the pill.
Why is my acne or my irregular cycle back?
The short answer is that the pill suppressed whatever it was originally prescribed to manage, and now that pattern is meeting daylight again. This is the “unmasking” idea. It is what conventional medicine misses when it waves you off, and what the wellness market hides when it sells you a “reset.”
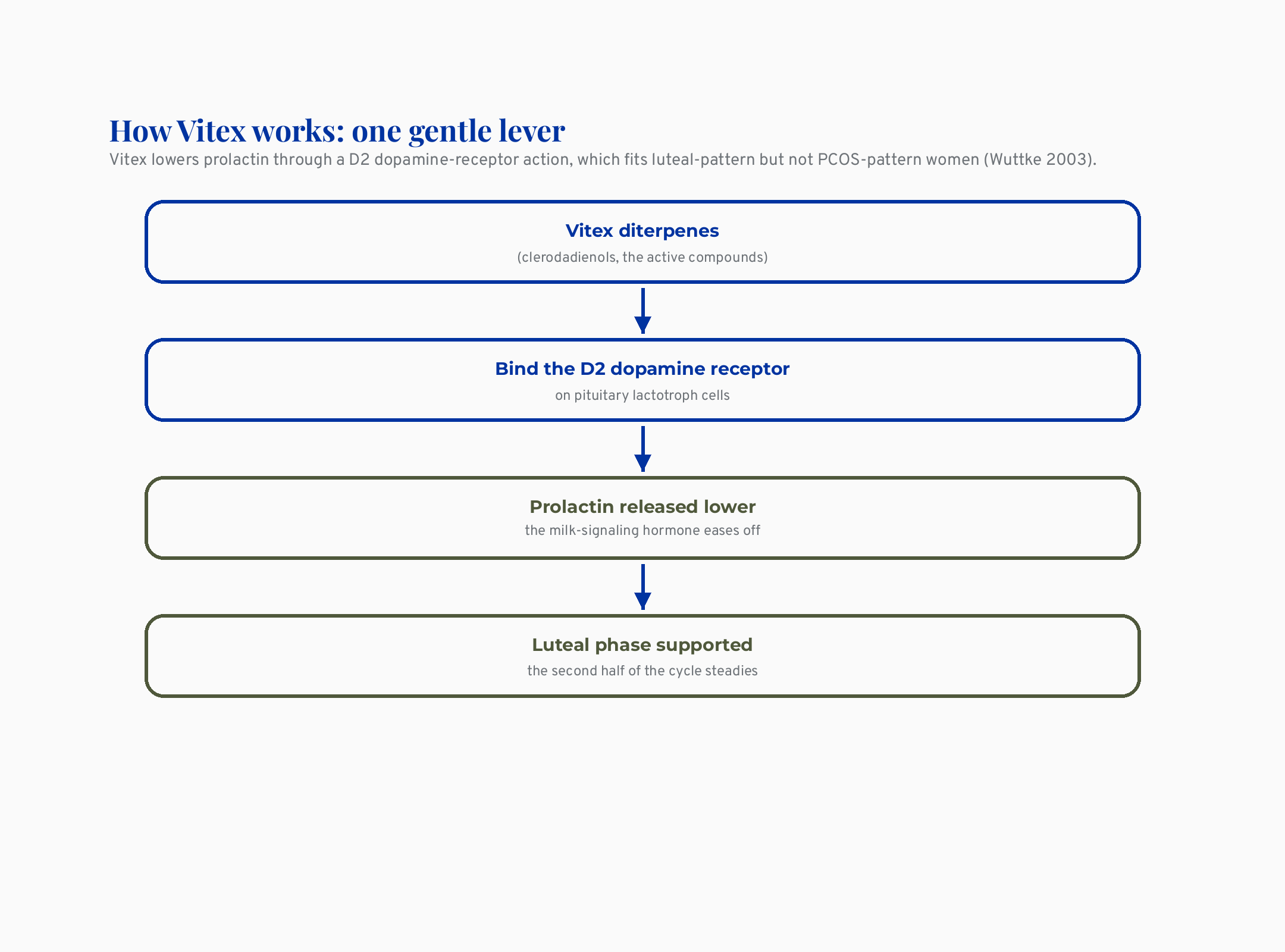
Think about why you were put on the pill in the first place. If it was for acne, oily skin, or irregular cycles, the driver underneath is often androgen-pattern, meaning higher activity of male-type hormones like testosterone. If it was for severe PMS, cyclic breast pain, or a short luteal phase, the driver is more often a prolactin-and-progesterone pattern. The luteal phase is the second half of your cycle, after ovulation. Prolactin is the hormone best known for milk production. When it runs a little high it can shorten that luteal phase and throw off your cycle.
I want to name a real example here, and her details are changed for confidentiality. A woman in her early thirties wrote to me convinced the pill had “given her PCOS.” Her acne and irregular cycles had roared back four months after stopping. In cases I have reviewed, that picture is almost always a pattern that predated the pill, briefly silenced by it, now returning. The pill did not write the question. It muted it.
For the woman reading this, the move is to ask what the pill was originally for, because that single answer reshapes everything that comes next.
What can I actually do to support my body off the pill?
Start with the unglamorous foundations, because they help nearly everyone and they carry the least risk. Replete the basics the pill can deplete, support your gut, and give your cycle real time. This is the part the influencer “detox” content skips because it does not sell a product.
The pill can lower some nutrients, including B vitamins, magnesium, and zinc, and vitamin D can dip after stopping. The evidence here is medium, some of it secondhand, so I will not oversell it. Repleting these is low-risk and reasonable, not magic.
Fiber and whole foods support estrogen clearance and the estrobolome, meaning the community of gut bacteria that helps recycle and clear estrogen from your body. This one is mechanistically reasonable but thin on hard outcome data, so I hold it gently. It is a sensible habit, not a cure. If you want the deeper version of how gut bacteria shape estrogen, my piece on why your probiotic isn’t working and which one might walks through strain specificity, which is the part most “gut reset” advice gets wrong.
And here is the honest one about time. No botanical has been tested in a defined post-pill population that I have found. Every herb claim in this space is borrowed from studies on PMS, PMDD, or high prolactin, not on women who just stopped the pill. That gap matters, and you deserve to know it exists. What this means for you: foundations and patience first, herbs second, and only the herb that matches your actual pattern.
Does Vitex help everyone after the pill?
No, and this is the single most important correction in the whole topic. Vitex, also called chaste tree, is not a universal post-pill herb. It fits one pattern well and can be the wrong tool for another, and the wellness market almost never tells you which is which.
Vitex lowers prolactin through a D2 dopamine-receptor action, which fits luteal-pattern but not PCOS-pattern women (Wuttke 2003). The D2 dopamine receptor is a docking site in the brain that controls prolactin release, and Vitex gently nudges it. That same mechanism is why Vitex suits the prolactin-and-short-luteal-phase woman. It can backfire for the androgen-pattern or PCOS woman, who is over-represented in the exact group coming off the pill.
So does it work at all? For PMS, yes, but with a real asterisk. Vitex beat placebo for PMS, but 91% study heterogeneity means that effect is likely overstated (Verkaik 2017). Heterogeneity means the studies disagreed with each other a lot. Paired with signs of publication bias, that is why the authors themselves called the pooled result “merely explorative.” So the honest read has three parts. Vitex genuinely helps some women. The effect is probably smaller than the headlines. And it is matched to a pattern, not sprinkled on everyone.
This is the same teaching I walk through in my black cohosh evidence audit: a beloved plant can have real mechanism, real tradition, and still have softer trial evidence than the bottle implies. Natural is not automatically safe or proven. For the woman reading this, the takeaway is that Vitex is a precision tool, not a blanket fix. Matching it to your pattern is the whole game.
Who should NOT take Vitex?
If you are pregnant or breastfeeding, you should avoid Vitex, full stop. Its dopamine action can suppress milk supply, and it is not a benign add-on. This is the safety line I will not soften.
Use real caution if you take dopamine-active medications, meaning drugs like bromocriptine, certain antipsychotics, or metoclopramide. Vitex acts on the same dopamine pathway, so the interaction is plausible. It is also the wrong tool for androgen-pattern and PCOS presentations, and for women in the middle of IVF. Altering prolactin and luteal hormones inside a controlled cycle is not something to improvise.
The PCOS overlap deserves its own flag, because the pill so often masks it. PCOS is the condition most likely to resurface when you stop, and it has even been getting a proposed new name. My evaluation of the PCOS-to-PMOS rebrand covers what actually changes for you and what does not.
One more honesty note: the trials ran for only a few cycles. Long-term safety beyond about six months is not well established, and I will not reassure you past the data. For the woman reading this, the rule is plain. If your picture looks androgen-driven, or you are pregnant, nursing, on dopamine-active meds, or doing IVF, Vitex is probably not your herb.
What I’d do this week
Here is the bookmarkable version, the decision map I would want a friend to have taped inside her cabinet. Save this one. It is education, not a prescription, and not a reason to stop or change your contraception.
The bottom line
The honest, root-cause read is the one neither side says plainly. The pill did not break your hormones, it hid the question. The most useful thing I can do is help you tell normal re-regulation apart from a pattern that was always there. The symptoms are real, the herbs can be reasonable, and the timeline plus the red-flag rule will tell you more than any single bottle.
If you have read this far, thank you. Which step on that map is the one you most needed to see today? Tell me, and I will keep making the honest version of this content for you.
Frequently asked questions
How long until my period comes back after stopping the pill? For most women the period returns within about three months as the HPO axis re-regulates, and roughly 80% re-regulate inside that window. If your period has not returned by three months, ask your provider for testing, including a pregnancy test, thyroid, and prolactin.
Is post-pill syndrome real? “Post-pill syndrome” is not a formal medical diagnosis, but the symptoms are real. They usually reflect either temporary re-regulation or the return of a condition the pill was masking, such as PCOS or painful periods. Naming it honestly is more validating, because it points to a cause instead of a vague reset.
Does Vitex help everyone after the pill? No. Vitex lowers prolactin through a dopamine-receptor action, so it fits prolactin-and-luteal-phase patterns and can backfire for androgen-pattern or PCOS presentations. It outperformed placebo for PMS in pooled trials, but high study heterogeneity means that effect is likely overstated. Match it to your pattern rather than reaching for it by default.
Can the pill damage my fertility? The evidence does not support lasting fertility damage from the pill itself. In a pooled analysis of 14,884 women, 83% conceived within a year off the pill regardless of how long they used it. When conceiving is harder, the usual cause is an underlying condition the pill was masking, not the years on it.
Who should NOT take Vitex? Avoid Vitex in pregnancy and breastfeeding, since its dopamine action can suppress milk supply. Use caution with dopamine-active medications like bromocriptine, antipsychotics, or metoclopramide, and avoid it during IVF and in androgen-pattern or PCOS presentations. Long-term safety beyond a few months is not well established.
What if my acne came back worse after stopping the pill? Returning acne usually means an androgen-pattern the pill was suppressing is resurfacing, not new damage. Zinc around 30 mg a day is the better-studied first move, and it is worth assessing for PCOS. Vitex is generally the wrong tool for this picture, so matching the support to the driver matters more than reaching for the most popular herb.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Girum, T., & Wasie, A. (2018). Return of fertility after discontinuation of contraception: A systematic review and meta-analysis. Contraception and Reproductive Medicine, 3, 9. https://doi.org/10.1186/s40834-018-0064-y
2. Wuttke, W., Jarry, H., Christoffel, V., Spengler, B., & Seidlova-Wuttke, D. (2003). Chaste tree (Vitex agnus-castus): Pharmacology and clinical indications. Phytomedicine, 10(4), 348-357. https://doi.org/10.1078/094471103322004866
3. Verkaik, S., Kamperman, A. M., van Westrhenen, R., & Schulte, P. F. J. (2017). The treatment of premenstrual syndrome with preparations of Vitex agnus castus: A systematic review and meta-analysis. American Journal of Obstetrics and Gynecology, 217(2), 150-166. https://doi.org/10.1016/j.ajog.2017.02.028
4. Csupor, D., Lantos, T., Hegyi, P., Benko, R., Viola, R., Gyongyi, Z., … Matuz, M. (2019). Vitex agnus-castus in premenstrual syndrome: A meta-analysis of double-blind randomised controlled trials. Complementary Therapies in Medicine, 47, 102190. https://doi.org/10.1016/j.ctim.2019.08.024
5. van Die, M. D., Burger, H. G., Teede, H. J., & Bone, K. M. (2012). Vitex agnus-castus extracts for female reproductive disorders: A systematic review of clinical trials. Planta Medica, 79(7), 562-575. https://doi.org/10.1055/s-0032-1327831
6. Puglia, L. T., Lowry, J., & Tamagno, G. (2023). Vitex agnus castus effects on hyperprolactinaemia. Frontiers in Endocrinology, 14, 1269781. https://doi.org/10.3389/fendo.2023.1269781
7. Dietz, B. M., Hajirahimkhan, A., Dunlap, T. L., & Bolton, J. L. (2016). Botanicals and their bioactive phytochemicals for women’s health. Pharmacological Reviews, 68(4), 1026-1073. https://doi.org/10.1124/pr.115.010843