Beyond the Hype: The 2026 Guide to Picking the Right Magnesium
1. Introduction: The Invisible Mineral Gap
While nearly half of the U.S. adult population (48%) fails to meet the estimated average requirement for magnesium through diet alone—according to the latest Babu & Krishnamurthy (2025) NHANES analysis—the "invisible mineral gap" remains a pervasive clinical failure. Most individuals seeking relief for anxiety, insomnia, or fatigue are supplementing with the wrong molecular forms and seeing zero results.
The problem is twofold: modern laboratory medicine relies on biomarkers that systematically ignore tissue depletion, and the supplement industry often prioritizes "elemental weight" over actual biological uptake. This guide distills the latest 2026 clinical research to help you move beyond marketing claims and select the specific molecule required for your physiology.
2. The Bioavailability Trap: Why Your Supplement Might Be Failing You
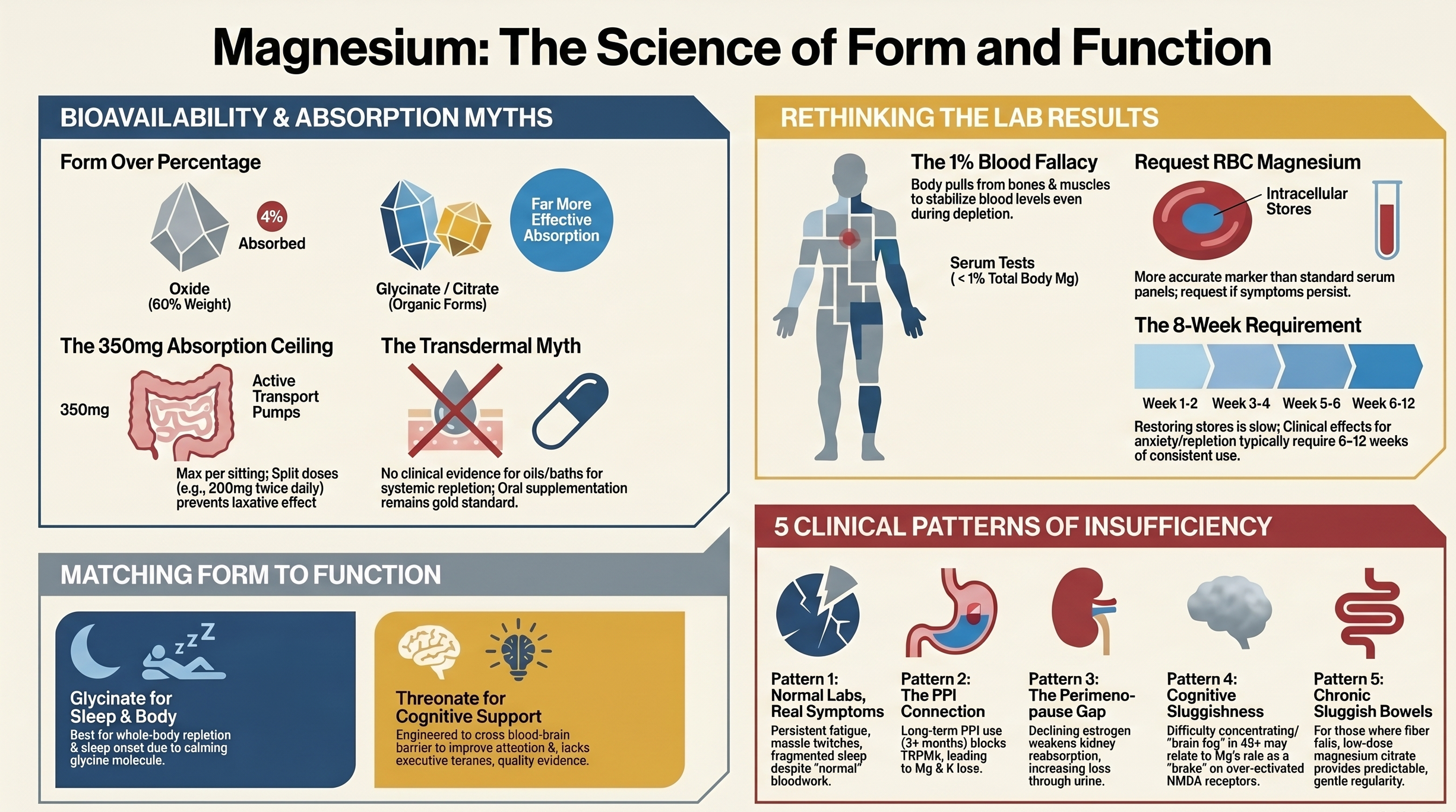
A common clinical frustration is the patient who remains symptomatic despite daily supplementation. This usually stems from the "bioavailability trap." There is a vast difference between the amount of magnesium in a pill (elemental weight) and the amount that survives the transit from your gut to your bloodstream (bioavailability).
Inorganic forms like Magnesium Oxide are frequently sold because they are inexpensive and dense. However, Oxide is essentially a "plumbing" supplement; its poor absorption makes it an effective saline laxative but a failure for systemic repletion. Conversely, organic chelates like Glycinate are designed to "hitchhike" on amino acid transporters for superior uptake.
Magnesium Form
Absorption Rate (Approximate)
Primary Clinical Use Case
Magnesium Oxide
~4%
Acute bowel preparation / Laxative
Magnesium Glycinate/Bisglycinate
80%+
Systemic repletion, sleep, anxiety
"Organic forms (glycinate, citrate, malate) are substantially more bioavailable... Magnesium oxide is appropriate only for acute bowel preparation or as an inexpensive laxative. It is not appropriate for systemic repletion." — Pardo et al. (2021)
Reflection: Relying on Oxide for systemic health is a financial and biological error. You are essentially paying for a expensive laxative effect while your muscles, heart, and brain remain starved for the mineral.
3. Glycinate vs. Threonate: Tissue vs. Transit
The two most discussed forms in 2026 are Glycinate and L-Threonate (MgT). While Glycinate is the "workhorse" for filling the body's general stores, Magnesium L-Threonate was engineered to cross the blood-brain barrier via specific transporters.
The Cognitive Signal: The landmark Lopresti & Smith (2026) RCT (n=100) investigated MgT's effects on the brain using the NIH Total Cognition Composite. Findings included:
An estimated 7.5-year reduction in "brain age."
Significant improvements in episodic memory and reaction times.
Increased synaptic density via NMDA receptor modulation.
A Note on Clinical Skepticism: It is critical to note that nearly the entire research chain for MgT—from the initial 2010 animal models to current human trials—has been funded or conducted by entities with industry affiliations (Neurocentria/Magceutics). Furthermore, while MgT is excellent for "brain fog," the 2026 trial found no significant objective sleep benefit for this form.
Can they be taken together? Yes. They are complementary. Glycinate ensures systemic saturation, while Threonate targets the central nervous system. However, given the cost, Threonate should be viewed as a premium cognitive tool, not a general repletion strategy.
4. The Sleep Selection: Why Glycinate Wins the Night
Marketing often pushes Threonate for sleep, but the data does not support this. For insomnia and sleep architecture, Magnesium Glycinate/Bisglycinate remains the gold standard.
The secret lies in the glycine co-ligand. Glycine is an inhibitory neurotransmitter that increases GABAergic activity, calming the central nervous system.
"Significant improvements in sleep time, sleep efficiency, and a 17-minute reduction in sleep onset latency were observed [with magnesium]." — Abbasi et al. (2012)
The Granular Truth: While the Mah & Pitre (2021/2024) meta-analysis confirmed the 17-minute reduction in how fast people fall asleep, it also noted that the increase in Total Sleep Time (TST) was not statistically significant. Magnesium helps you get into sleep, but it isn't a "knockout" pill that guarantees an extra two hours of rest.
5. Anxiety and the "Slow-Burn" Effect
Magnesium acts as a physiological "brake" by occupying the NMDA receptor to prevent excitatory over-firing and increasing GABA-A receptor sensitivity. It also regulates the HPA (stress) axis, preventing a "runaway" cortisol response.
The Repletion Timeline: Unlike a sedative, magnesium requires tissue repletion to stabilize mood. Clinical signals for anxiety typically emerge after 6–12 weeks of consistent use. A one-week trial is biologically insufficient to judge its efficacy for the nervous system.
6. The GI Equation: Solving Constipation Without the Chaos
Magnesium Citrate is highly effective for motility because of its osmotic effect—it draws water into the colon. However, taking too much at once causes "laxative overflow."
Clinical Protocol: The Dose Titration Guide
Target: Magnesium Citrate (moderate-to-high bioavailability with a gentle pro-motility effect).
Starting Dose: 150–200mg of elemental magnesium.
Timing: Bedtime only.
Adjustment: If stools are too loose, reduce by 50mg. If no movement occurs, increase by 50mg every third night until a natural rhythm is established.
7. The Perimenopause Connection: The Estrogen-Magnesium Link
Perimenopause is a period of high magnesium vulnerability. As estrogen levels decline, the kidneys lose their efficiency at retaining minerals—a process known as renal magnesium wasting (driven by reduced TRPM6 channel expression).
A Necessary Reality Check: While the mechanistic link between estrogen loss and magnesium depletion is sound, the "hype" around magnesium for hot flashes requires caution. The NCCTG N10C2 Phase 3 RCT, a large placebo-controlled trial, found no significant difference between magnesium and placebo for hot flash frequency. While magnesium is essential for the mood and sleep disruption of the transition, it is not a primary "cure" for vasomotor symptoms.
8. Dosing Intelligence: The 350mg Rule
Magnesium absorption is "saturable"—your TRPM6/TRPM7 transporters can only process so much at once. Taking 400mg in one sitting often results in the excess remaining in the gut, causing GI distress rather than systemic benefit.
Best Practices:
Split Dosing: Take 150-200mg in the AM and PM to maximize total daily uptake.
Target Elemental Weight: Aim for ~350mg of elemental supplemental magnesium daily.
Watch for Depletors: Long-term use of Proton Pump Inhibitors (like Omeprazole) or loop diuretics (like Furosemide) can cause severe, chronic depletion that requires professional monitoring.
9. The Testing Lie: Why "Normal" Isn't Enough
Standard serum magnesium tests are notoriously insensitive because less than 1% of your body's magnesium is in the blood. Your body will "leach" magnesium from your bones and muscles to keep serum levels stable for heart function, meaning your blood work can look "perfect" while your tissues are starving.
Superior Alternatives:
RBC Magnesium: Measures levels within red blood cells; a much better proxy for tissue stores.
24-Hour Urinary Load Test: Measures how much magnesium you excrete after a dose. If your body retains a high percentage, it confirms a baseline deficiency.
10. Honorable Mentions: Malate and Taurate
Magnesium Malate: Often favored for energy and fibromyalgia, as malic acid is a key player in the Krebs cycle (ATP production).
Magnesium Taurate: Emergent research suggests this form may be superior for cardiovascular tone and heart rhythm due to the synergistic effect of taurine.
11. Conclusion: A Targeted Approach to Minerals
The core takeaway of the 2026 research is that form dictates function. Magnesium is not a monolith; it is a delivery system for specific health outcomes.
For Sleep & Anxiety: Choose Glycinate.
For Brain Power & Memory: Choose Threonate.
For Digestion: Choose Citrate.
If your lab results say you are "normal," but your body is telling you that you are exhausted, anxious, and unable to sleep, which one will you trust?
Disclaimer
This content is for educational purposes only and is not intended to diagnose, treat, or replace individualized medical care. Please consult your physician or qualified healthcare provider before making changes to your health, especially if you have a medical condition or are taking medications.
FAQ
For frequently asked questions on magnesium, refer to this page: Magnesium: Which Form Does What
References
[1] National Institutes of Health, Office of Dietary Supplements. (2024). Magnesium: Fact sheet for health professionals. https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/
[2] Pardo, M. R., Garicano Vilar, E., San Mauro Martín, I., & Camina Martín, M. A. (2021). Bioavailability of magnesium food supplements: A systematic review. Nutrition, 89, 111294. PMID: 34111673 https://doi.org/10.1016/j.nut.2021.111294
[3] [Non-peer-reviewed commercial URL removed from formal reference list. Osmotic laxative mechanism of Mg citrate/oxide is established in primary pharmacology literature; claims in this document are supported by refs 1, 2, and 16.]
[4] Slutsky, I., Abumaria, N., Wu, L.-J., Huang, C., Zhang, L., Li, B., Zhao, X., Govindarajan, A., Zhao, M.-G., Zhuo, M., Tonegawa, S., & Liu, G. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron, 65(2), 165–177. PMID: 20152124 https://doi.org/10.1016/j.neuron.2009.12.026
[5] Sun, Q., Weinger, J. G., Mao, F., & Liu, G. (2016). Regulation of structural and functional synapse density by L-threonate through modulation of intraneuronal magnesium concentration. Neuropharmacology, 108, 426–439. PMID: 27178134 https://doi.org/10.1016/j.neuropharm.2016.05.006
[6] Lopresti, A. L., & Smith, S. J. (2026). The effects of magnesium L-threonate (Magtein®) on cognitive performance and sleep quality in adults: A randomised, double-blind, placebo-controlled trial. Frontiers in Nutrition, 12, 1729164. PMID: 41601871 https://doi.org/10.3389/fnut.2025.1729164
[7] Babu, N., & Krishnamurthy, S. (2025). Global dietary magnesium deficiency: Prevalence, underlying factors, health implications, and strategic interventions. International Journal of Vitamin and Nutrition Research, 95(6). https://doi.org/10.31083/IJVNR46828
[8] Florentin, M., & Elisaf, M. S. (2012). Proton pump inhibitor-induced hypomagnesemia: A new challenge. World Journal of Nephrology, 1(6), 151–154. PMC: 3782221 https://doi.org/10.5527/wjn.v1.i6.151
[9] Guerrero-Romero, F., & Rodríguez-Morán, M. (2011). Magnesium improves the beta-cell function to compensate variation of insulin sensitivity: Double-blind, randomized clinical trial. European Journal of Clinical Investigation, 41(4), 405–410. PMID: 21241290 https://doi.org/10.1111/j.1365-2362.2010.02422.x
[10] Murck, H. (2002). Magnesium and affective disorders. Nutritional Neuroscience, 5(6), 375–389. PMID: 12509067 (Narrative review; used for mechanistic framing only. Note: Taylor & Francis online date 2013 reflects digitization date; original print year is 2002 per PubMed.) https://doi.org/10.1080/1028415021000039194
[11] Mah, J., & Pitre, T. (2021). Oral magnesium supplementation for insomnia in older adults: A systematic review and meta-analysis. BMC Complementary Medicine and Therapies, 21(1), 125. PMID: 33865376 https://doi.org/10.1186/s12906-021-03297-z
[12] Park, H., Parker, G. L., Boardman, C. H., Morris, M. M., & Smith, T. J. (2011). A pilot phase II trial of magnesium supplements to reduce menopausal hot flashes in breast cancer patients. Supportive Care in Cancer, 19(6), 859–863. PMC: 3085555 https://doi.org/10.1007/s00520-011-1099-7
[13] Boyle, N. B., Lawton, C., & Dye, L. (2017). The effects of magnesium supplementation on subjective anxiety and stress — A systematic review. Nutrients, 9(5), 429. PMID: 28445426 https://doi.org/10.3390/nu9050429
[14] Castiglioni, S., Cazzaniga, A., Albisetti, W., & Maier, J. A. (2013). Magnesium and osteoporosis: Current state of knowledge and future research directions. Nutrients, 5(8), 3022–3033. PMID: 23912329 https://doi.org/10.3390/nu5083022
[15] Choudhary, R., Bodakhe, S. H., & Gupta, S. K. (2018). Magnesium taurate attenuates progression of hypertension and cardiotoxicity against cadmium chloride-induced hypertensive albino rats. Journal of Traditional and Complementary Medicine, 8(4), 466–473. PMC: 6435948 https://doi.org/10.1016/j.jtcme.2017.09.004
[16] Schuchardt, J. P., & Hahn, A. (2017). Intestinal absorption and factors influencing bioavailability of magnesium — An update. Current Nutrition and Food Science, 13(4), 260–278. (Narrative review; used for dose-saturation and split-dosing rationale) https://doi.org/10.2174/1573401313666170427162740
[17] Guerrero-Romero, F., Jaquez-Chairez, F. O., & Rodríguez-Morán, M. (2016). Magnesium in metabolic syndrome: A review based on randomized, double-blind clinical trials. Magnesium Research, 29(4), 146–153. PMID: 27917820 (Replaces prior duplicate entry; context: metabolic syndrome and insulin resistance.) https://doi.org/10.1684/mrh.2016.0404
[18] Moabedi, M., Aliakbari, M., Erfanian, S., & Milajerdi, A. (2023). Magnesium supplementation beneficially affects depression in adults with depressive disorder: A systematic review and meta-analysis. Frontiers in Psychiatry, 14, 1333261. PMID: 38213402 https://doi.org/10.3389/fpsyt.2023.1333261
[19] Abbasi, B., Kimiagar, M., Sadeghniiat, K., Shirazi, M. M., Hedayati, M., & Rashidkhani, B. (2012). The effect of magnesium supplementation on primary insomnia in elderly: A double-blind placebo-controlled clinical trial. Journal of Research in Medical Sciences, 17(12), 1161–1169. PMID: 23853635 https://pubmed.ncbi.nlm.nih.gov/23853635/
[20] Barbagallo, M., & Dominguez, L. J. (2010). Magnesium and aging. Current Pharmaceutical Design, 16(7), 832–839. PMID: 20388094 https://doi.org/10.2174/138161210790883679
[21] Cleveland Clinic. (2023). Hypomagnesemia: What it is, causes, symptoms & treatment. (Non-primary; clinical summary; used for symptom/etiology context) https://my.clevelandclinic.org/health/diseases/23264-hypomagnesemia
[22] Kirkland, A. E., Sarlo, G. L., & Holton, K. F. (2018). The role of magnesium in neurological disorders. Nutrients, 10(6), 730. PMID: 29882776 https://doi.org/10.3390/nu10060730
[23] Tarleton, E. K., Littenberg, B., MacLean, C. D., Kennedy, A. G., & Daley, C. (2017). Role of magnesium supplementation in the treatment of depression: A randomized clinical trial. PLOS ONE, 12(6), e0180067. PMID: 28654669 https://doi.org/10.1371/journal.pone.0180067
[24] Schwalfenberg, G. K., & Genuis, S. J. (2017). The importance of magnesium in clinical healthcare. Scientifica, 2017, 4179326. PMID: 29093983 https://doi.org/10.1155/2017/4179326