Why 16:8 Fasting May Be Too Short (And What Works)
If you have been told 16:8 is the safe, gentle version of fasting, and you have spent the last year trying to make it work while your period gets weird and your sleep gets thinner and your hair shows up everywhere except on your head, I want you to stop blaming your discipline. The data shifted in 2025. The largest US cohort analysis to date on eating windows showed a U-shaped curve, meaning eating windows that are too short and eating windows that are too long both raise mortality risk. The safest zone for most adults sat around 11 to 12 hours per day. This piece will walk you through what the evidence actually says, where the wellness world has overshot, the specific timing lever that matters more than how hard you fast, and the drug-timing problem nobody is talking about when an eating window collapses. Here is what I will cover: the U-curve, the early-versus-late distinction, what happens to women’s hormones when fasting goes too far, a practical “what I would do this week” save card, and when this tool is not the right tool for you.
Is my eating window actually too short?
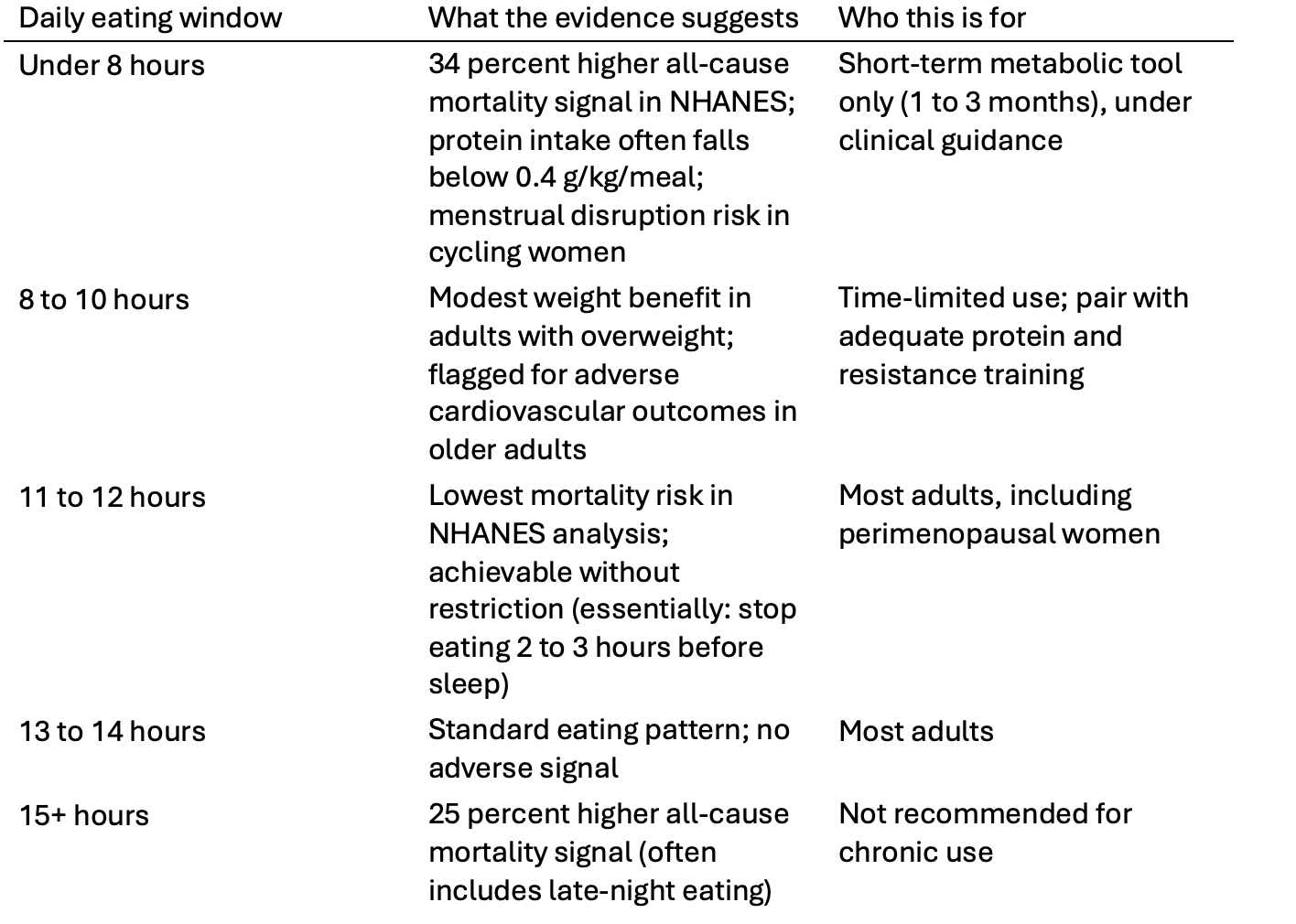
If you find yourself counting hours instead of food and still feeling worse, the question worth asking is not “am I disciplined enough?” but “am I past the dose where this still helps?” For many adults, the answer is yes. The current evidence supports a U-shaped relationship between daily eating window and all-cause mortality, with the lowest risk around 11 to 12 hours. Windows under 8 hours per day were associated with 34 percent higher all-cause mortality in a 2025 NHANES analysis of more than 33,000 US adults (Mao et al., Aging Cell). Windows of 15 hours or more were associated with a 25 percent higher signal. The shape is U, not a straight line.
That is a real reframe. The wellness conversation has treated “shorter eating window = better” as if it were linear. The largest dataset to date now disagrees.
Micro-summary: The new cohort data shows a U-shape. Too short and too long both raise mortality signals. The safest middle is around 11 to 12 hours.
What this means for the woman in front of me is simple. If your last bite is at 8 pm and your first bite is at 8 am, that is a 12-hour overnight gap. That single shift captures most of the cardiometabolic benefit the chrononutrition (timing-of-eating) literature supports. You do not have to skip breakfast. You do not have to white-knuckle through lunch. You just have to stop eating before bed.
What is the U-curve, and why does it matter for women in their 30s and 40s?
The U-curve is the shape of the mortality risk when you plot it against daily eating window. Both extremes carry risk. The middle is safer.
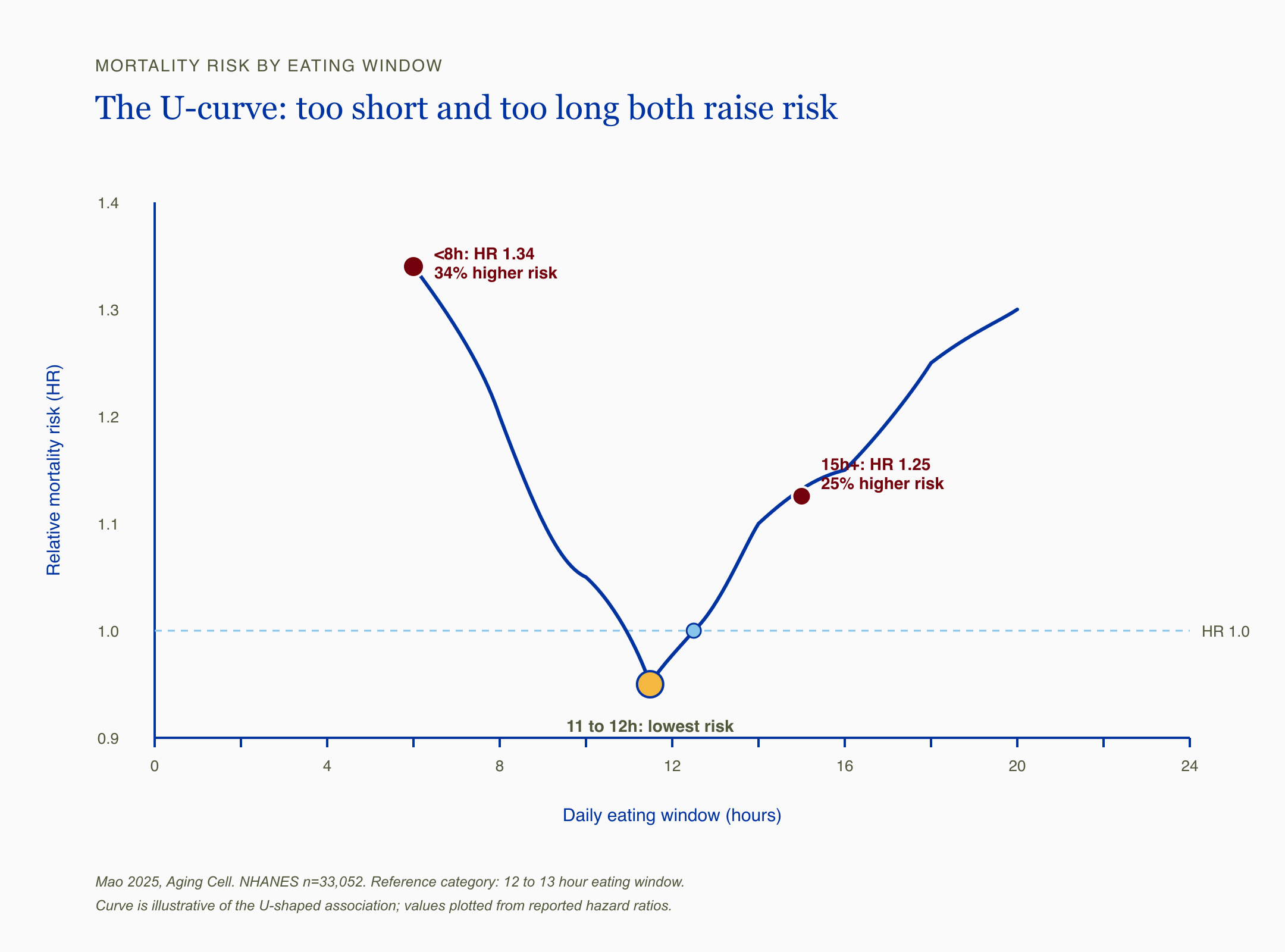
U-shaped mortality curve from Mao 2025 NHANES analysis showing lowest risk at 11 to 12 hour eating windows, with elevated risk at less than 8 hours and at 15 hours or more
Eating windows under 8 hours per day showed 34 percent higher all-cause mortality versus 12 to 13 hour windows (Mao 2025, NHANES n=33,052).
Read that sentence twice. The reference category, the one with the lowest mortality, was a 12 to 13 hour eating window. Not 8 hours. Not 6 hours. Twelve hours.
For women in their 30s and 40s, this matters for reasons the influencer space rarely names. The Mao analysis is observational, which means it cannot prove causation. A serious skeptic would point out that people who happen to eat within an 8-hour window on the recall days may be sicker, older, or living with food insecurity. That critique is fair and worth holding. The evidence here is strong as a signal, not as proof of cause. But the practical takeaway does not depend on causation. A 12-hour overnight gap is conservative, easy to hit, and consistent with every other line of chrononutrition evidence including the NHLBI 2023 workshop synthesis.
I had a friend in her late thirties tell me she had been doing 16:8 for fourteen months, was exhausted by 3 pm every day, had lost her cycle for the second time, and was convinced something was structurally wrong with her thyroid. Her thyroid panel came back unremarkable. The variable that had changed was that she was eating dinner at 4:30 and snacking on almonds at 11 pm to “get her last calories in.” She was technically inside her 8-hour window. She was also eating two hours before bed. The window was not the lever. The timing was.
Micro-summary: The U-curve says both very short and very long eating windows carry risk. For women 33 to 45, the 11 to 12 hour window is the sweet spot, and the time you finish eating matters more than the total window length.
Why “16:8 is the safe one” is incomplete advice
The 16:8 protocol was marketed as the gentle entry-level fast. It is not categorically harmful. The 2026 Couto-Alfonso network meta-analysis in older adults found 16:8 produced modest weight loss without lean mass loss when combined with adequate protein and resistance training. That is real benefit. The trouble starts when 16:8 is sold as a universal longevity tool to a 38-year-old woman whose cortisol is already running hot and whose protein intake is already on the floor.
Isocaloric 8-hour eating windows did not improve insulin sensitivity in women with overweight over two weeks (Peters 2025, Science Translational Medicine, n=31).
That is the cleanest single trial in this exact population. Researchers in Germany ran a randomized crossover where women with overweight ate the same number of calories either in an early 8-hour window (8 am to 4 pm) or a late 8-hour window (1 pm to 9 pm). When calories were matched, neither window improved insulin sensitivity, 24-hour glucose, lipids, or markers of oxidative stress. The “timing alone, without eating less, fixes your metabolism” claim did not hold up.
This is the part of the conversation that gets lost. Most weight loss on 16:8 happens because people quietly eat less when they have fewer hours to do it in. That is fine as a 1 to 3 month metabolic tool. It is not the same thing as “the eating window itself is doing the work.” When you take the calorie deficit away, the metabolic benefit goes with it. The mechanism story is more nuanced than the marketing.
Micro-summary: 16:8 can produce modest benefit, but when calories are held constant, an 8-hour window alone did not improve insulin sensitivity in women with overweight. The deficit, not the timing, is doing most of the work.
The early-eating vs late-eating distinction
Here is the thing the chrononutrition literature has converged on. Insulin sensitivity is highest in the morning and declines through the day. Eating a larger share of calories earlier aligns nutrient intake with peak diurnal sensitivity. Late-night eating, on the other hand, asks an insulin-resistant body to handle a glucose load.
That is why early time-restricted eating (eTRE, which means finishing your eating window in the earlier part of the day) consistently outperforms late time-restricted eating (lTRE) in glycemic outcomes across multiple small RCTs. The eTRE pattern aligns with the NHLBI 2023 chrononutrition workshop synthesis published in JAHA in 2025, which endorses earlier eating and avoiding late-night eating without prescribing a specific eating window.
What this means for the woman in front of me, who is working a real job and parenting and trying not to skip dinner with her family, is not “you must finish eating by 3 pm.” The practical anchor is gentler than that. Finish eating 2 to 3 hours before sleep. If you go to bed at 10 pm, that means last bite around 7 to 8 pm. That single shift covers most of the chrononutrition signal without rebuilding your day.
I have seen women try to push that anchor to its extreme and end the eating window at 4 pm because someone on Instagram said earlier was better. They were hungry, cranky, and not sleeping. The early-eating principle is a vector, not a finish line. Pulling dinner earlier by even an hour or two captures most of the benefit.
Micro-summary: Earlier eating beats later eating for cardiometabolic outcomes. The practical anchor is finishing dinner 2 to 3 hours before bed, not skipping dinner entirely.
What happens to your hormones when fasting goes too far
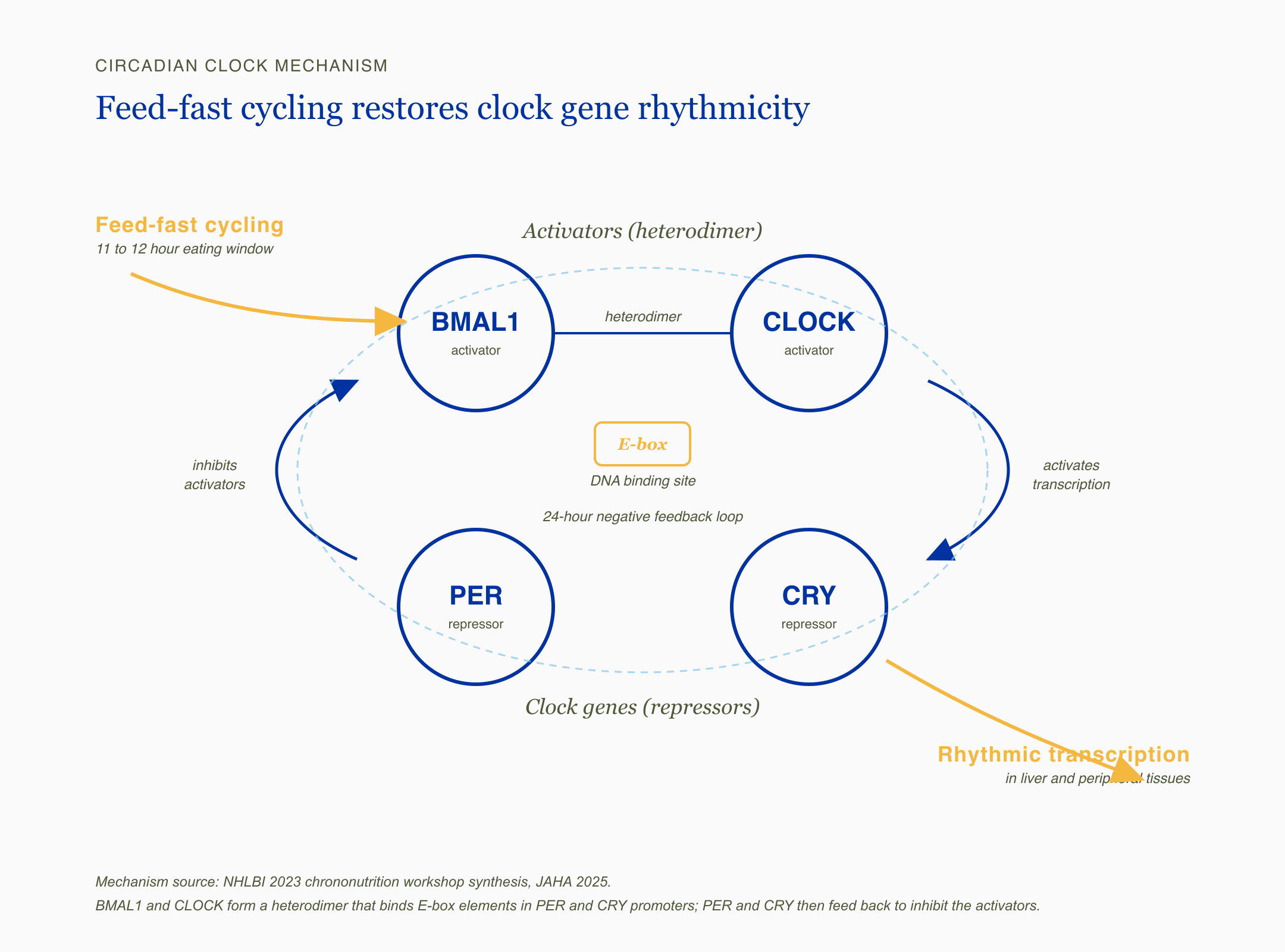
Diagram of the circadian clock gene feedback loop showing BMAL1 and CLOCK forming a heterodimer that binds an E-box DNA element and activates transcription of PER and CRY, which feed back to inhibit BMAL1 and CLOCK, with feed-fast cycling driving rhythmic transcription in liver and peripheral tissues
If your period got weird, if your hair started shedding, if your sleep collapsed three months into 16:8, you are not imagining the connection. Your body is reporting back.
Cycling women have an HPA axis (hypothalamic-pituitary-adrenal, the brain-to-adrenal stress system) and a reproductive axis that talk to each other constantly. Sustained energy deficit and prolonged fasting can downregulate kisspeptin (a hypothalamic signal that controls GnRH pulses and therefore your menstrual cycle), which then quiets the entire reproductive cascade. This is the mechanism behind functional hypothalamic amenorrhea, the clinical name for losing your period because your brain stopped sending the signal.
The mechanism is well established. The exact dose at which 16:8 TRE (time-restricted eating, the clinical term) produces clinically meaningful kisspeptin suppression in a free-living perimenopausal woman is not. RCT evidence in this specific population is still missing. What I have is mechanism plus what I have seen in cases I’ve reviewed: women in their late thirties and early forties are the most vulnerable cohort to “I followed the protocol and I got worse.”
The second issue is protein. Muscle protein synthesis (MPS, the process by which your body builds and maintains muscle) becomes harder to trigger as you move past 40. The dose-response evidence suggests women over 40 need roughly 0.4 grams of protein per kilogram of body weight per meal to maximize MPS. For a 150-pound woman, that is about 27 grams of protein per meal. Compressed into an 8-hour window with only two meals, you have one shot at hitting that target twice. Most women I have talked to about this are eating closer to 15 grams per meal. Over months, that compounds into lost lean mass and softer bone density.
Micro-summary: Aggressive fasting can suppress reproductive signaling, disrupt the cortisol curve, and compress protein intake below the dose women over 40 need for muscle and bone preservation. The mechanism is robust. RCTs in this exact population are still pending.
The pattern I have seen is that the women who feel best on fasting are not the ones with the shortest windows; they are the ones whose last bite is at 7 pm and whose body got a real overnight rest."
The drug-timing problem nobody talks about
This is where the wellness conversation goes silent. If you are on a thyroid medication, a diabetes medication, or a GLP-1 (glucagon-like peptide-1, the class that includes Ozempic, Wegovy, Mounjaro, and Zepbound), an 8-hour eating window changes your pharmacology and almost nobody mentions it.
Levothyroxine (the standard thyroid hormone replacement) has to be taken on an empty stomach 30 to 60 minutes before food. If your eating window starts at noon, your levothyroxine dose has to land at 11:00 or 11:30 at the latest. If you wake up at 6 am and take the pill then, you have to wait six hours to eat or you absorb less of the dose. Most women working a real schedule end up either skipping the morning dose or eating too close to it, which means absorption drops and the dose effectively shrinks. I have seen TSH numbers drift in exactly this pattern in cases I’ve reviewed.
Metformin (the first-line type 2 diabetes medication) is dosed with food specifically to reduce gastrointestinal side effects. An 8-hour window collapses your dosing options. Doses get skipped. Tolerance drops.
Sulfonylureas and insulin carry a serious hypoglycemia (low blood sugar) risk in a compressed eating window. This is not a “be a little careful” caveat. This requires medical supervision.
GLP-1 agonists are the harder conversation. These medications already drive caloric reduction by slowing gastric emptying and dampening appetite. Layering an 8-hour eating window on top can accelerate lean mass and bone density loss because the total caloric intake collapses faster than your body can adapt. The protein dose per meal becomes near-impossible to hit. If you are on a GLP-1, the chrononutrition lever you want is the 12-hour overnight gap, not a compressed window.
Micro-summary: If you are on levothyroxine, metformin, insulin, a sulfonylurea, or a GLP-1, a short eating window changes how the medication works. The 12-hour window is the safer chrononutrition tool in any of these cases, and the GLP-1 conversation specifically requires clinician supervision.
What I’d do this week
Here is the bookmarkable artifact. Save this card, screenshot it, send it to the friend who has been white-knuckling 16:8 for a year.
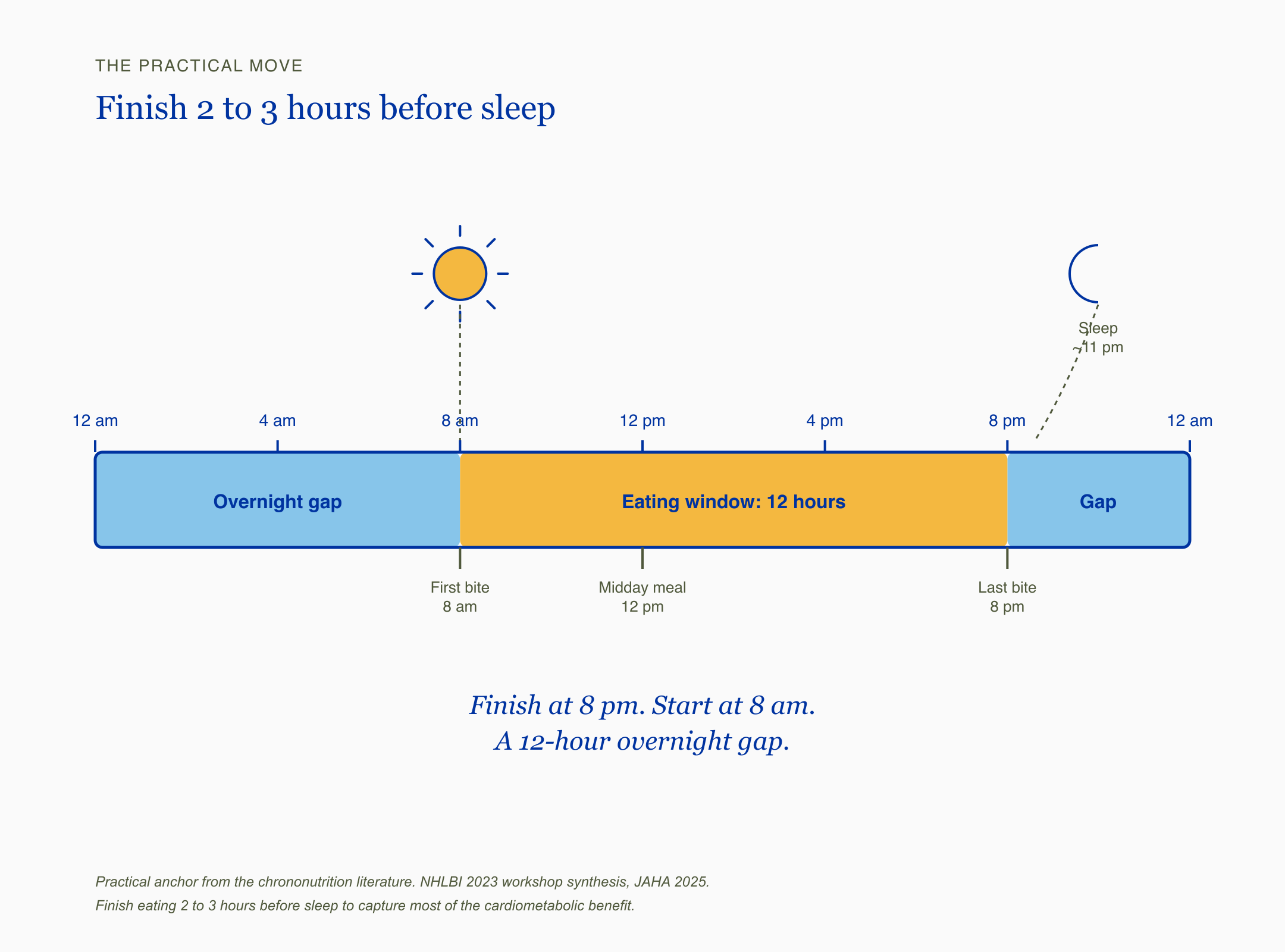
A 24-hour timeline showing a 12-hour eating window from 8 am to 8 pm in Gold, with the overnight gap from 8 pm to 8 am in Sky Blue, anchored by a sun icon at 8 am and a moon icon at 11 pm, and the takeaway "Finish at 8 pm. Start at 8 am. A 12-hour overnight gap."
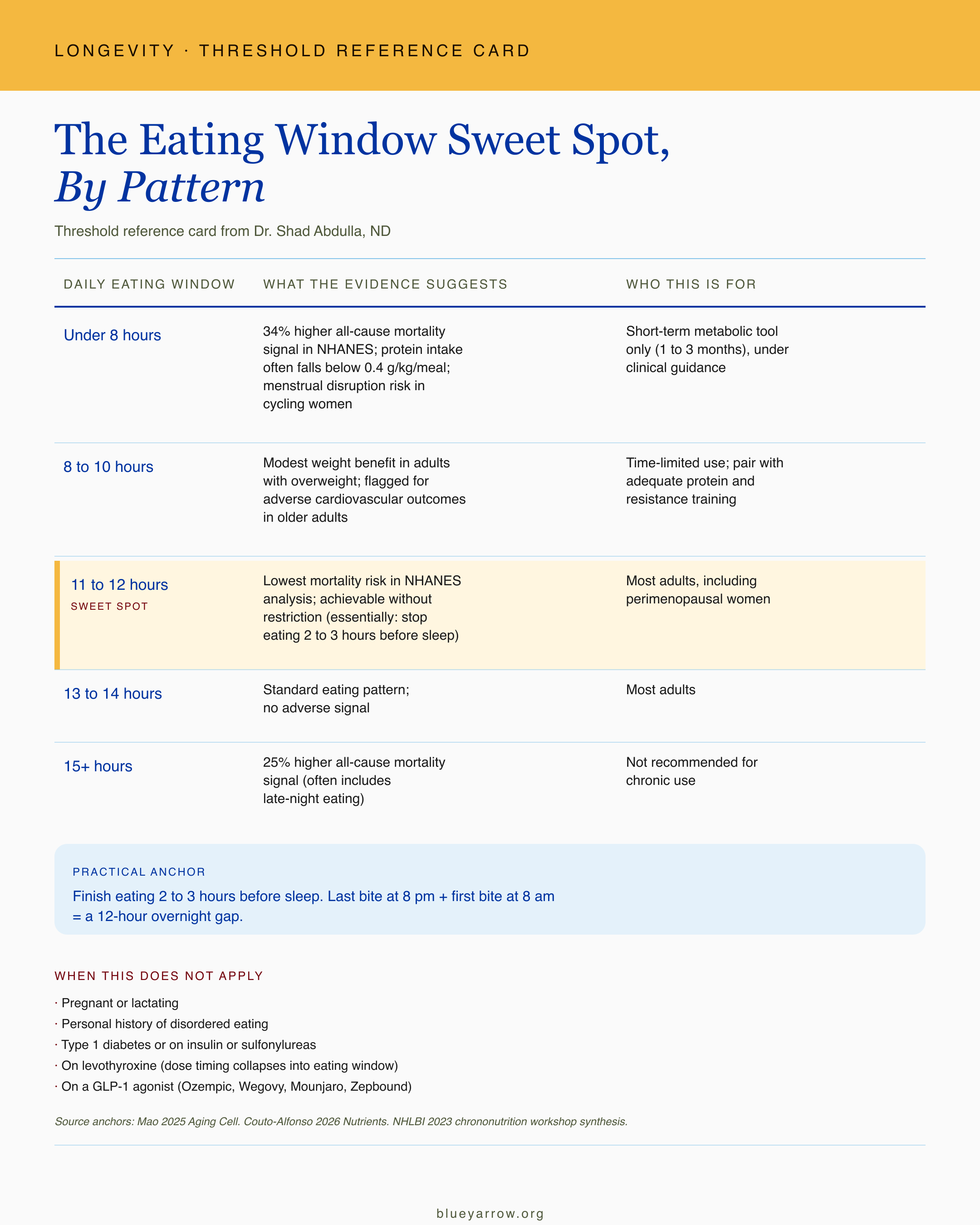
The Eating Window Sweet Spot, By Pattern
Practical anchor: Finish eating 2 to 3 hours before sleep. If your last bite is at 8 pm and your first bite is at 8 am, that is a 12-hour overnight gap. That single shift captures most of the cardiometabolic benefit the chrononutrition literature supports.
When this table does not apply: - Pregnant or lactating: any structured fasting is contraindicated. - Personal history of disordered eating: this is not a fasting tool to use without a clinician who knows your history. - Type 1 diabetes, or on insulin or sulfonylureas: hypoglycemia risk requires medical supervision. - On levothyroxine: dose timing collapses into the eating window. Sequence the dose 30 to 60 minutes before the first bite. - On a GLP-1 agonist (Ozempic, Wegovy, Mounjaro, Zepbound): caloric reduction is already happening. Layering fasting on top can accelerate lean mass and bone density loss.
This week, the experiment I would suggest if you want to try the lightest possible version is this. Pick a finish-eating time that is 2 to 3 hours before your normal bedtime. Hold it for two weeks. Track sleep quality and morning energy. If you have a cycle, track that. If you are on any of the medications above, talk to your prescribing clinician before changing your eating timing.
Micro-summary: The 11 to 12 hour window is the practical target. The single move is to finish eating 2 to 3 hours before sleep. That captures most of the benefit without restriction.
When this is not the tool for you
Eating windows of 10 hours or less were associated with 58 percent higher cardiovascular mortality in older adults versus standard windows (Couto-Alfonso 2026, Nutrients).
That signal in older adults is part of why this tool is not universal. There are populations for whom any structured fasting protocol is the wrong call, and naming them matters more than the protocol itself.
If you are pregnant or lactating. Structured fasting is contraindicated. The Pradella 2024 systematic review of Ramadan exposure in pregnancy found offspring health effects that travel into childhood and adulthood. The fetal programming concerns are real.
If you have a history of disordered eating, active or in remission. Please do not use this content as a fasting protocol. Anything that adds rigid rules around food can be a trigger. A clinician who knows your history is the right partner for any meal-timing change, and chrononutrition can be approached through “finish eating before bed” without ever framing it as fasting.
If you have type 1 diabetes, or are on insulin or sulfonylureas. The hypoglycemia risk is not theoretical. This requires medical supervision.
If you are 65 or older. The Couto-Alfonso 2026 review flagged restrictive eating windows in older adults specifically. The protein and bone density concerns compound with age. The 11 to 12 hour window is fine. The 8-hour window is not the right tool here.
If you are an active perimenopausal woman. This is the cohort where the wellness pressure is highest and the evidence is most cautious. The mechanism reasons to be careful are strong. RCT evidence in this specific population is still missing. What I have seen in cases I’ve reviewed is that the 12-hour overnight gap delivers most of the benefit without the cortisol and kisspeptin downside.
Micro-summary: Pregnancy, lactation, disordered eating history, type 1 diabetes, insulin or sulfonylurea use, age 65+, and active perimenopause are all flags where short fasting windows are not the right tool. The 11 to 12 hour overnight gap is.
The bigger frame is the one Blue Yarrow keeps coming back to. Fasting is a tool with a dose. Like any tool with a dose, more is not better past a point. The evidence here is strong enough to say the U-curve is real. It is not strong enough to say “8 hours will hurt you.” What it does say, clearly, is that the easiest, lowest-risk, highest-yield chrononutrition move is to finish eating before bed. If that is the only thing you take from this piece, you have what you need.
What is the one thing about your current eating pattern you want to change first?
Frequently asked questions
Is 16:8 intermittent fasting safe for women? The evidence is mixed and depends on context. 16:8 produced modest weight loss in adults with overweight in a 2026 meta-analysis when paired with adequate protein and resistance training. The 2025 NHANES analysis flagged windows under 8 hours with a 34 percent higher all-cause mortality signal. For perimenopausal women, mechanism reasons for caution exist, and RCT evidence in that specific cohort is still missing.
What is the best eating window for longevity? The largest US cohort analysis to date (Mao 2025, n=33,052) found the lowest mortality risk at 11 to 12 hours per day. Windows under 8 hours and over 15 hours both showed higher mortality signals. The practical translation is to finish eating 2 to 3 hours before sleep, which produces about a 12-hour overnight fast naturally.
Can fasting cause my period to stop? Sustained energy deficit and aggressive fasting can downregulate kisspeptin signaling in the hypothalamus, which can disrupt or stop menstrual cycles. This is the mechanism behind functional hypothalamic amenorrhea. If your period changed after starting a fasting protocol, the protocol is a reasonable thing to revisit with a clinician.
Is early time-restricted eating better than late? Yes, based on current evidence. Insulin sensitivity is highest in the morning and declines through the day. Multiple RCTs show early time-restricted eating produces better glycemic outcomes than late time-restricted eating. The practical move is shifting dinner earlier rather than skipping breakfast.
Should I do intermittent fasting if I am on levothyroxine? Levothyroxine must be taken on an empty stomach 30 to 60 minutes before food. A compressed eating window often causes timing collapse and reduced absorption. An 11 to 12 hour window with the dose taken 30 to 60 minutes before your first bite preserves absorption. Talk to your prescribing clinician before changing your eating timing.
Can I do intermittent fasting on a GLP-1 medication like Ozempic? GLP-1 medications already drive caloric reduction. Layering a short eating window on top can accelerate lean mass and bone density loss because total intake and per-meal protein both fall. The chrononutrition lever to consider on a GLP-1 is the 12-hour overnight gap, not a compressed window. This conversation belongs with your prescribing clinician.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
Couto-Alfonso, S., Cenit, M. C., Sanz-Perez, C. M., & Iguacel, I. (2026). Intermittent fasting and healthy aging in older adults: A systematic review of cardiometabolic, mental health and cognitive outcomes with a network meta-analysis of anthropometric measures. Nutrients, 18(9), 1450. https://doi.org/10.3390/nu18091450
Mao, Z. et al. (2025). Association of eating window with mortality among US adults: Insights from a nationally representative study. Aging Cell.https://doi.org/10.1111/acel.70230
Peters, B., Schwarz, J., Schuppelius, B., et al. (2025). Intended isocaloric time-restricted eating shifts circadian clocks but does not improve cardiometabolic health in women with overweight. Science Translational Medicine, 17(822), eadv6787. https://doi.org/10.1126/scitranslmed.adv6787
Pradella, F., Witte, P., & van Ewijk, R. (2024). Ramadan during pregnancy and offspring health outcomes over the life course: A systematic review and meta-analysis. Human Reproduction Update, 30(6), 789-812. https://doi.org/10.1093/humupd/dmae026
Advancing chrononutrition for cardiometabolic health: A 2023 National Heart, Lung, and Blood Institute workshop report. (2025). Journal of the American Heart Association.https://doi.org/10.1161/JAHA.124.039373
Popiolek-Kalisz, J., & Kwasny, A. (2025). The impact of intermittent fasting on lipid profile: An umbrella review. Nutrition, Metabolism & Cardiovascular Diseases, 36(3), 104472. https://doi.org/10.1016/j.numecd.2025.104472
National Institute for Health and Care Excellence. (2025). Overweight and obesity management (NICE guideline NG246). https://www.nice.org.uk/guidance/ng246