Pepcid & Claritin for Perimenopause: What Actually Helps
If you have been scrolling Threads or TikTok and watching a wave of women say a fifteen-dollar OTC drug stack handed them their brain back, you are not imagining it. Women in their late thirties and early forties are reporting that a daily second-generation antihistamine plus famotidine cleared brain fog, quieted intrusive thoughts, settled food reactions, and made them feel like themselves again. Then they took the post to their doctor and got a blank stare or a dismissal. Both responses are missing the story.
Here is what I want to do in this post. I want to walk you through the biology, which is real and is not made up by influencers. I want to give you a five-symptom screen so you can tell if this angle even applies to you. I want to name the part of hot flashes the trend gets wrong, and the part of histamine biology the medical guidelines have not caught up on yet. I want to lay out the safety questions your pharmacist should be raising and is not. And then I want to give you a clear sense of what I would actually do this week if I were the woman holding the box at the pharmacy. If you want to skim, the headers are written so you can read just the bolded answers and still leave with the framework.
What's actually happening with estrogen, histamine, and mast cells
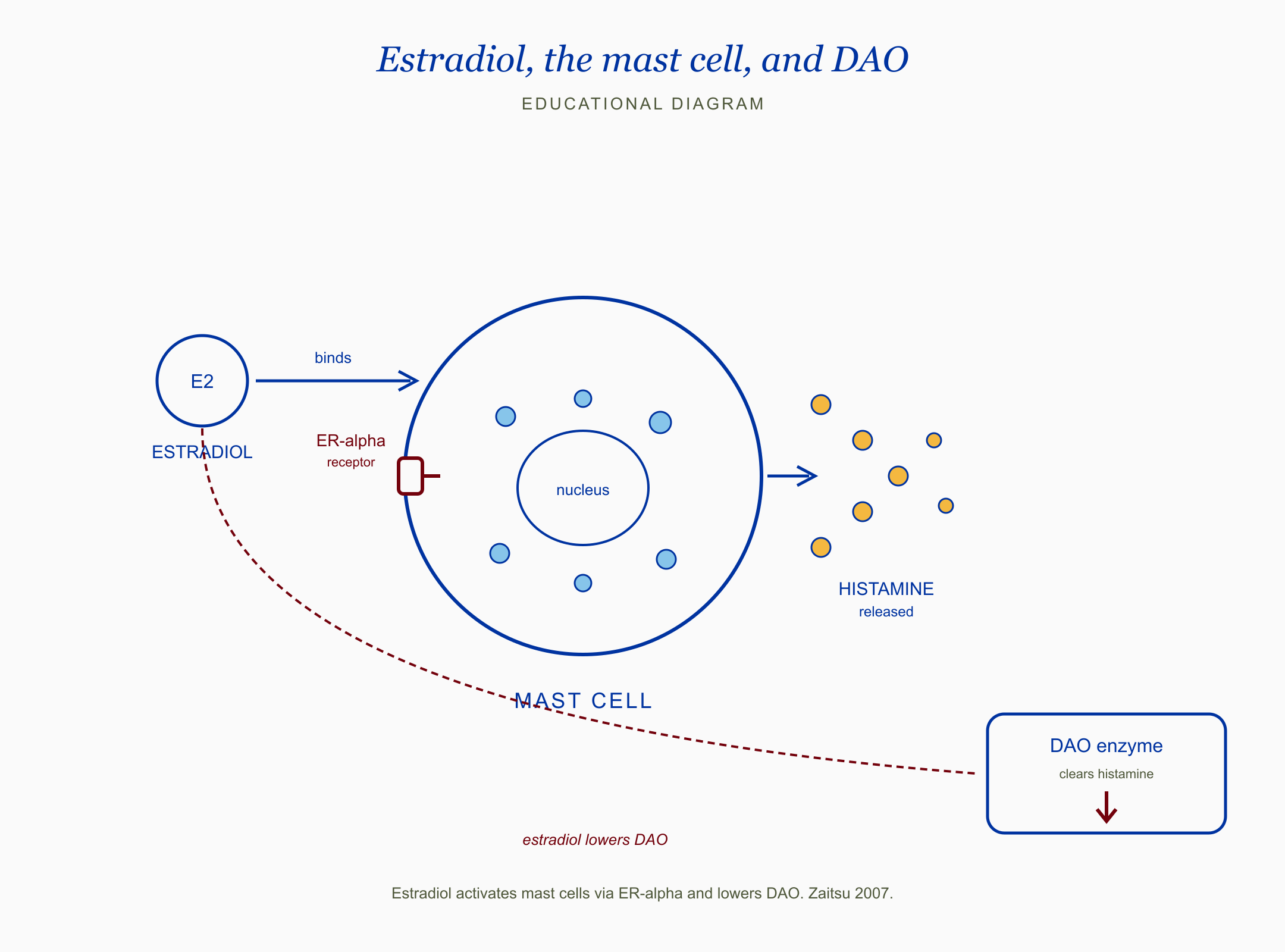
Diagram showing estradiol binding ER-alpha on a mast cell, triggering histamine release, and a separate arrow indicating estradiol lowers the DAO enzyme that clears histamine. Citation: Zaitsu 2007.
The short answer: estrogen and histamine talk to each other, and in perimenopause that conversation gets noisy.
Estrogen activates mast cells, which are the immune cells that store and release histamine, the same molecule that drives allergy symptoms. Estradiol activates mast cells via ER-alpha and lowers DAO, the enzyme that clears histamine, per Zaitsu 2007. ER-alpha is one of the two main estrogen receptors. DAO stands for diamine oxidase, the enzyme your gut makes to break down dietary histamine. When estradiol (the strongest form of estrogen) goes up, mast cells get twitchier and the body has a harder time clearing the histamine that gets released. Progesterone does the opposite. It stabilizes mast cells and supports DAO. This part comes from mechanistic work in the 2000s and a comprehensive 2024 sex-hormone-and-allergy review (full citations in the references list).
Here is why this matters in perimenopause specifically. Progesterone tends to decline earlier than estradiol. Estradiol does not glide downward, it spikes and crashes in increasingly erratic patterns through the late thirties and early forties. That creates windows of relative estrogen excess against a falling progesterone backdrop, which is the exact biochemistry where mast cells get more reactive and histamine clears more slowly.
If you have been told for years that your symptoms are anxiety, your doctor was not necessarily wrong about what you were feeling. They were wrong about why.
The micro-summary so far: estrogen makes mast cells more active and slows histamine clearance. Progesterone calms mast cells and supports clearance. Perimenopause disrupts that balance before estrogen drops.
Why hot flashes are mostly hypothalamic, not histamine
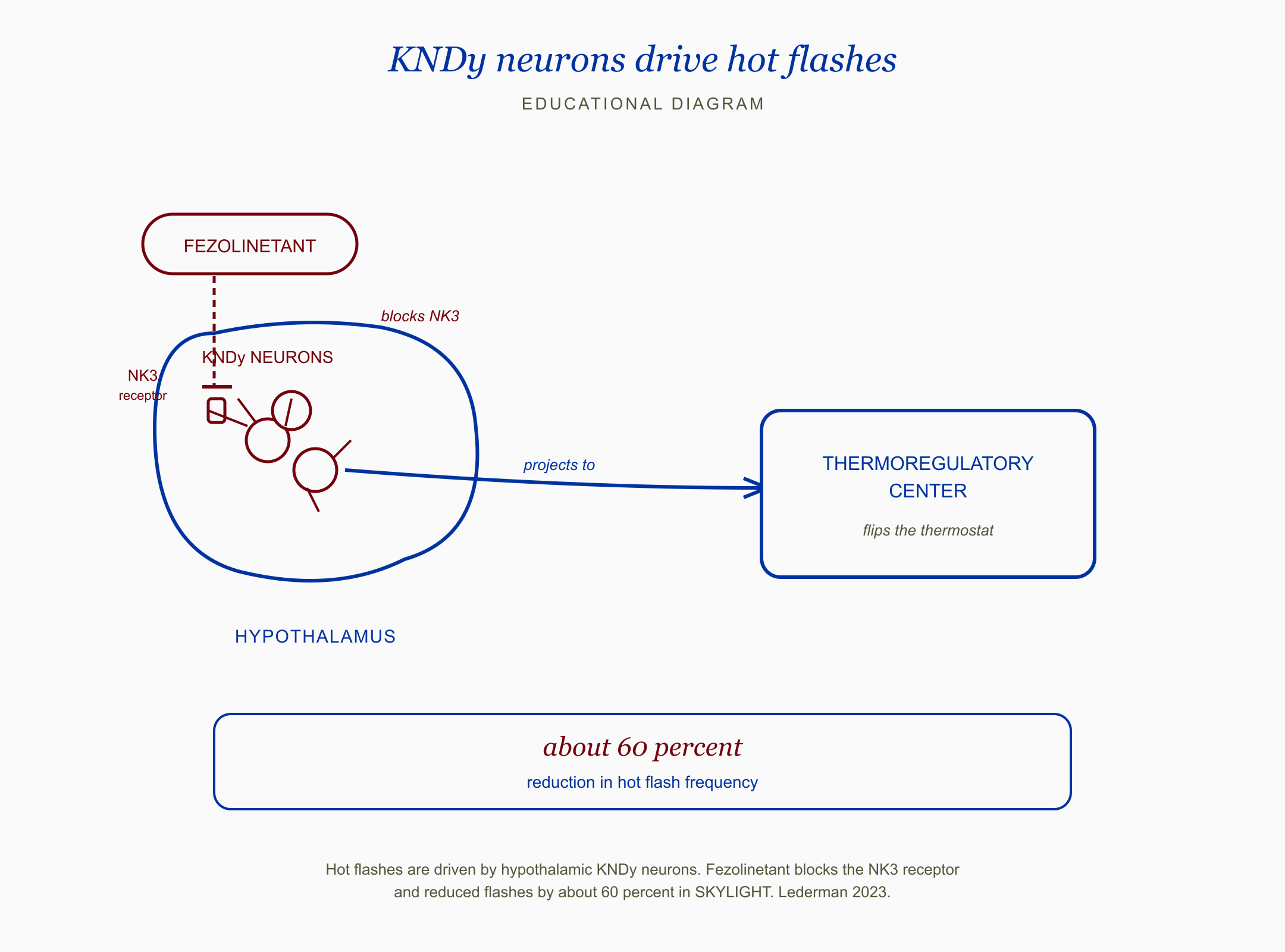
Schematic of the hypothalamus showing KNDy neurons projecting to the thermoregulatory center, with fezolinetant blocking the NK3 receptor on the KNDy neuron, plus a result panel reading about 60 percent reduction in hot flash frequency. Citation: Lederman 2023 SKYLIGHT.
The short answer: true vasomotor hot flashes come from your brain, not your mast cells. This is where the trend gets cited badly.
Hot flashes are driven by hypothalamic KNDy neurons, which is why fezolinetant cuts them about 60 percent (Lederman 2023, SKYLIGHT). KNDy stands for kisspeptin, neurokinin B, and dynorphin, the three signaling molecules these neurons use. They sit in the arcuate nucleus of the hypothalamus, right next to the thermoregulatory center, which is the part of the brain that decides whether to make you sweat. When estrogen withdraws, these neurons get bigger and fire harder, which is what flips the thermostat. Fezolinetant (brand name Veozah) is a drug that blocks this pathway, and it cuts hot flash frequency by close to 60 percent in the phase 3 SKYLIGHT trials.
That is the cleanest piece of evidence I have read that the central driver of hot flashes is upstream in the brain, not downstream in peripheral mast cells. A small 1976 human study looked at this directly. Estrogen relieved hot flushes in the women studied but did not change histamine turnover. The hot flash relief did not flow through histamine.
So if your dominant symptom is the classic vasomotor hot flash, the climbing wave of heat followed by the dump and the sweat, and you do not have the other histamine-pattern stuff, an antihistamine stack is unlikely to be the lever that moves the needle for you. Hormone therapy or fezolinetant target the actual mechanism. This is what I want a woman holding the Pepcid box to understand before she starts a six-month experiment.
The interesting part of the trend is not the hot flash claim. It is that some women report dramatic relief in the things that are not hot flashes, the brain fog, the food reactions, the joint pain, the cycle-correlated mood crashes. That is where the biology fits.
Who this combination actually helps, and who it doesn't: a 5-symptom screen
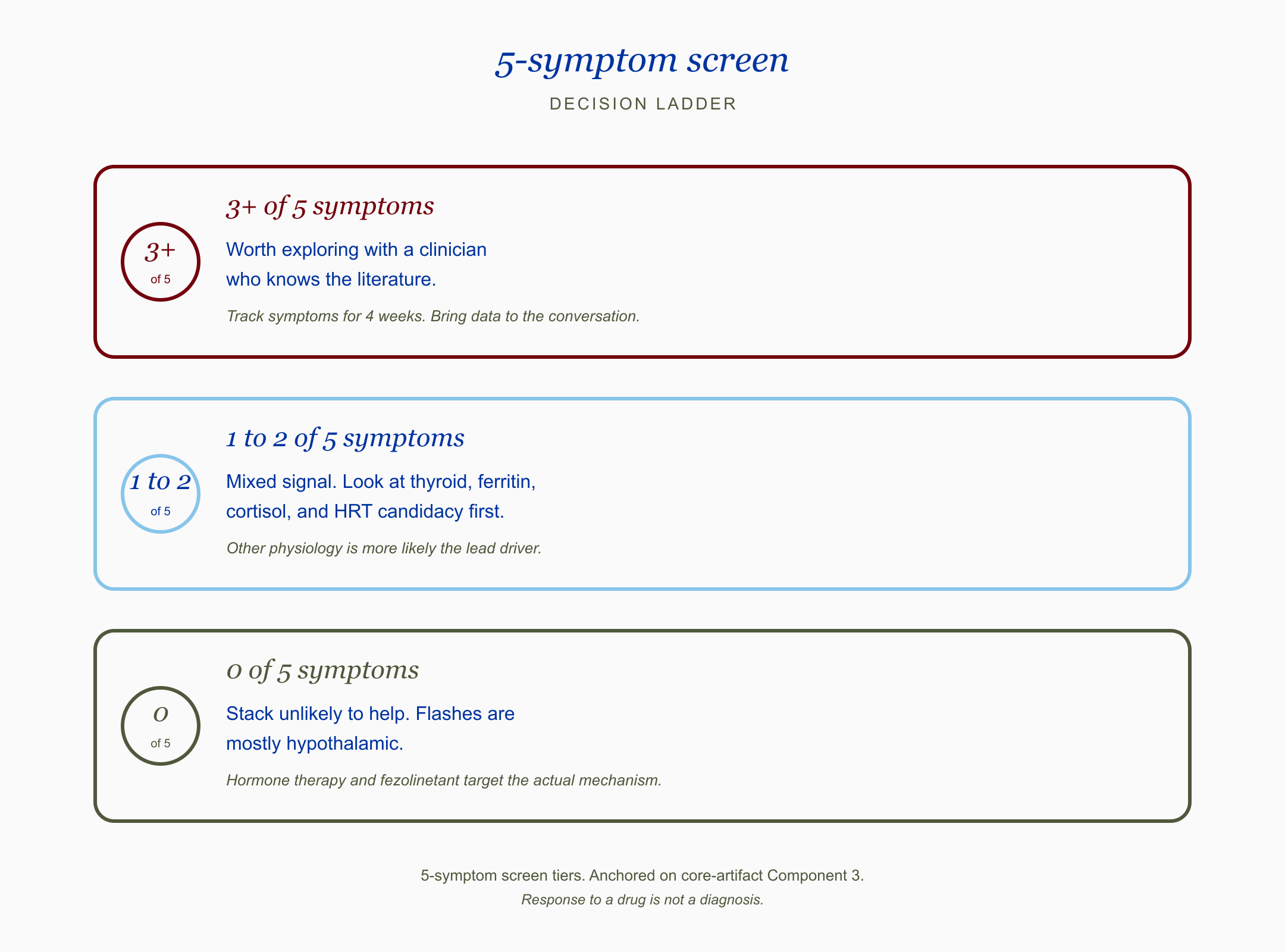
Three-tier decision ladder for the 5-symptom screen: 3 or more symptoms in Crimson worth exploring with a clinician, 1 to 2 symptoms in Sky Blue as a mixed signal pointing to thyroid, ferritin, cortisol, and HRT candidacy, 0 symptoms in Olive where the stack is unlikely to help and flashes are mostly hypothalamic.
The short answer: there is a pattern, and if you do not fit the pattern, this stack is probably not your lever.
I have read the same case series and the same Reddit and Threads testimonials a lot of you have. The women who report the most dramatic responses share a cluster of features that overlap with what is described in chronic urticaria, interstitial cystitis case series, and PMDD literature. The cluster is not a validated diagnostic test. The trials have not been run yet. I do find it clinically useful as a working screen for whether the histamine angle is worth a real look. The screen has five items.
What this means for the woman in front of me: I am not handing her a label. I am handing her a way to decide if the experiment is worth running with eyes open, and what to track if she runs it.
Track yourself for the last six to twelve months against these five items:
New food reactions. Wine, aged cheese, leftovers, fermented foods, or chocolate now flush, itch, bloat, or give you a headache where they did not before.
Flushing or rosacea pattern. Not the climbing-and-gone hot-flash wave. A longer pink flush across the cheeks, neck, or chest, often tied to food, heat, alcohol, or stress.
Hives, itch, or burning skin. Random hives that come and go. Itchy scalp. Skin that feels sunburned for no obvious reason.
Cycle-correlated mood crash. Anxiety, irritability, or intrusive thoughts that spike in the second half of the cycle and lift when you bleed.
Histamine-pattern insomnia. Falling asleep is fine. Waking at 2 to 4 a.m. wired, hot, or itchy is the problem.
If three or more of those fit, the histamine angle is worth a real conversation with a clinician who knows the literature. Track symptoms for four weeks. Bring the data.
If one or two fit, you have a mixed signal. Other physiology is more likely the lead driver. Thyroid, ferritin, cortisol pattern, and HRT candidacy belong at the top of the workup, not antihistamines.
If none fit, this stack is unlikely to help you. Vasomotor symptoms alone, without the cluster, are mostly hypothalamic. The evidence-based comparators are hormone therapy and fezolinetant.
Caveat row that no influencer is saying out loud: feeling better on antihistamines does not mean you have histamine intolerance or MCAS. Mast cell activation syndrome is a formal diagnosis with multi-organ criteria and objective lab confirmation. Histamine intolerance has no validated biomarker. Response to a receptor blocker is information. It is not a diagnosis.
The HRT and histamine paradox
The short answer: hormone therapy can either help histamine-pattern symptoms or worsen them depending on which hormone and which route.
This is the nuance nobody is naming and it is the most useful clinical detail in the file. Estradiol is the form of estrogen used in most HRT formulations. It is also the form that activates mast cells most directly. So a woman with a strong histamine-pattern symptom cluster who starts oral or transdermal estradiol can occasionally feel worse in the first weeks. Pink cheeks deeper. Hives flaring. Sleep worse instead of better. She tends to be told it is "adjustment" and to push through. Sometimes it is. Sometimes the mast cell axis is the missing piece.
Oral micronized progesterone (the bioidentical form, brand name Prometrium) is the part of HRT that often gets framed as the protective add-on for the uterus. It is more than that biologically. Progesterone directly stabilizes mast cells and supports DAO. For some women, getting the progesterone right is what makes the estradiol tolerable.
That is the paradox in a sentence. The same hormone replacement strategy that is first-line for vasomotor symptoms can worsen histamine-pattern symptoms in the subset of women whose mast cells were already reactive. The 2025 Menopause Society guidelines reaffirm hormone therapy as first-line for women under 60 or within 10 years of menopause onset without contraindications. That positioning is correct and I do not want anyone reading this and concluding that antihistamines are a substitute for HRT in a woman who is a candidate. They are not.
What this means for the woman in front of me: if she is on HRT and has new or worsening histamine-pattern symptoms, the conversation is not "stop HRT." The conversation is "is the progesterone dosed and routed right, and is there a mast cell layer underneath that deserves attention?"
What antihistamines actually do (and don't do)
The short answer: they block receptors. They do not lower histamine.
This is the language error I want to retire. Antihistamines block H1 and H2 receptors. They do not reduce how much histamine your body makes or improve how fast you clear it, per pharmacology basics. H1 receptors live on blood vessels, smooth muscle, and skin nerves, which is why H1 blockers (Allegra, Claritin, Zyrtec) help itch, hives, flushing, and runny nose. H2 receptors live primarily on stomach parietal cells, which is why H2 blockers (Pepcid, also called famotidine) lower stomach acid. H2 receptors also exist in the brain and on immune cells, which is part of why famotidine has been studied in adjacent conditions.
The reason the H1 plus H2 combination got popular is that some symptoms in this cluster, especially brain fog and mood symptoms, seem to track better with H2 blockade than H1 alone. There is a single small randomized trial of famotidine 40 mg twice daily in post-COVID adults with documented cognitive impairment that showed significant cognitive score improvement at 12 weeks against placebo. That is not a perimenopause study and it does not generalize. It is suggestive of why women might add the H2 blocker rather than just take the H1. The trials in the actual target population have not been run yet.
There are also two small women's case series in the adjacent literature. One used cetirizine plus famotidine in interstitial cystitis. The other used loratadine plus famotidine in urinary frequency. Both showed substantial symptom relief in women whose conditions sit on the mast cell axis. Small numbers, no controls, but consistent with mechanism. I see this consistently in cases I have reviewed, that the strongest responders look more like these adjacent phenotypes than like the textbook hot-flash patient.
The trend's language of "I lowered my histamine" is wrong. The accurate version is "I blocked the receptors that translate histamine into the symptoms I was feeling." If the receptors come back online and the underlying mast cell reactivity has not been addressed (sleep, alcohol, stress, hormone status, gut), the symptoms return.
Safety: what your pharmacist should be telling you and isn't
The short answer: this is not a free ride, especially long-term, and there are interactions almost nobody flags.
I want to walk through the safety layer specifically because the conventional coverage of this trend either skipped it or buried it in a final paragraph that nobody read.
Long-term H2 blockade is not benign. Chronic famotidine use reduces gastric acid, which is the upstream step for absorbing vitamin B12 and iron. B12 deficiency causes neurological symptoms (numbness, brain fog, mood changes) that look exactly like the symptoms the trend is meant to treat, which is the kind of irony that becomes a clinical problem on a 24-month timeline. Iron deficiency drives fatigue, restless legs, and hair shedding. If you are going to run this stack daily for more than a few months, getting B12, ferritin, and a CBC checked annually is the floor.
Famotidine has two drug interactions worth naming. Tizanidine is a muscle relaxer used in chronic pain and post-injury syndromes. Famotidine can raise tizanidine levels, which can drop blood pressure and cause sedation. Most prescribers know this. Most pharmacists flag it. Some do not. The other is ketoconazole and a few other antifungals, plus pH-dependent drugs like atazanavir and oral iron supplements. Famotidine raises gastric pH and reduces absorption of these. The fix is usually separation by several hours, not avoidance.
The dementia question is the one people ask me most. The answer is: it depends entirely on which antihistamine. The well-documented dementia signal is for first-generation antihistamines like diphenhydramine (Benadryl) and doxylamine (Unisom). These have heavy anticholinergic activity, and cumulative exposure over a decade was associated with a meaningfully increased dementia risk in the Gray 2015 JAMA Internal Medicine cohort study. If you are reaching for Benadryl for sleep on top of a daily Pepcid plus Claritin stack, that is the part I would change first.
The second-generation H1 antihistamines in the trend (loratadine, cetirizine, fexofenadine) carry far less anticholinergic burden. The dementia data for them, and for H2 blockers like famotidine, is mixed. One older cohort found a famotidine signal in older African American adults. More recent analyses, including a 2023 Mass General report, did not replicate it. I read that as a watch-and-wait, not a do-not-take. I am not over-warning here because the evidence does not support that.
The bigger long-term concern, in my read, is the masking problem. Chronic famotidine can mask reflux that is actually an early gastric cancer in women over 40. Chronic H1 blockade can mask chronic spontaneous urticaria that has an underlying autoimmune trigger that deserves a workup. Women who self-prescribe for years without medical follow-up risk missing both.
For pregnancy and lactation: loratadine, cetirizine, fexofenadine, and famotidine all have reassuring data per LactMed monographs. Loratadine and fexofenadine are the preferred H1 choices during breastfeeding. None of them have an associated congenital malformation signal in the available cohorts. That part of the safety conversation is in better shape than the long-term self-prescribing part.
I have read the same paper in three rooms now. The biology is real. The trend is not the protocol.
The bolded micro-summary: short-term, this stack is well-tolerated in healthy adults. Long-term, the unsexy issues are B12, iron, drug interactions, and masking. The dementia issue is real for first-gen H1s and unsettled for the rest.
What I'd do this week
The short answer: if you fit the cluster, run a structured four-week observation. If you do not, redirect your attention to what the evidence supports for your actual symptom pattern.
This is not a prescription. It is the framework I would want a woman to bring into a real conversation with a clinician. The save card below is the bookmarkable version. Screenshot it.
Does the histamine angle apply to you? A 5-symptom screen
Tick the boxes that describe you in the last 6 to 12 months.
New food reactions. Wine, aged cheese, leftovers, fermented foods, or chocolate now flush, itch, bloat, or trigger headache where they did not before.
Flushing or rosacea pattern. Not the brief hot-flash wave that climbs and goes. A pinker, longer flush of the cheeks, neck, or chest, often tied to food, heat, alcohol, or stress.
Hives, itch, or burning skin. Random hives. Itchy scalp. Skin that feels like it is sunburned for no reason.
Cycle-correlated mood crash. Anxiety, irritability, or intrusive thoughts that spike in the second half of the cycle and lift with bleeding.
Histamine-pattern insomnia. Falling asleep is not the problem. Waking at 2 to 4 a.m. wired, hot, or itchy is.
3 of 5 or more: the histamine angle is worth exploring with a clinician who knows the literature. Track symptoms for 4 weeks. Bring data to the conversation.
1 or 2 of 5: mixed signal. Other physiology is more likely the lead driver. Look at thyroid, ferritin, cortisol pattern, and HRT candidacy first.
0 of 5: this stack is unlikely to help. Hot flashes alone, without the cluster, are mostly hypothalamic. Hormone therapy and fezolinetant target the actual mechanism.
Caveat row. Response to a drug is not a diagnosis. Feeling better on antihistamines does not mean you have histamine intolerance or MCAS. It means the receptor blockade quieted a downstream signal. The framework above is a clinical screen, not a label.
A second clinical observation worth naming here. The women I have read about who report the most dramatic responses are not the textbook 52-year-old with classic hot flashes. They are often 37 to 42, still cycling, with a luteal-phase mood crash and food reactions that started in the last two years, who have been worked up for anxiety and told their labs are normal. Placebo response accounts for 27 to 52 percent of hot flash relief in pooled trials, per Sherman 2014 meta-analysis. I hold that number in mind for every testimonial I read. Expectancy is a real force in this domain. Open-label placebos work for hot flashes. None of that erases the biology. It just means a personal experiment is what it is, not a verdict on mechanism.
If you decide to run the experiment, the questions worth asking your own clinician are about dosing duration, baseline labs (B12, ferritin, CBC, thyroid, fasting iron), interactions with anything else you take, and a check-in calendar. If you are on HRT or considering it, the progesterone-and-mast-cell layer is the underdiscussed conversation worth raising specifically.
When to actually talk to a doctor
The short answer: now, if any of these are on the list, and definitely before you cross the six-month mark of daily use.
You do not need permission to walk into a pharmacy and pick up an OTC drug. You do need a clinician in the loop if any of the following apply. New onset reflux in a woman over 40 deserves an evaluation, not a year of self-blocking acid. Hives that are daily, lasting longer than six weeks, are chronic spontaneous urticaria until proven otherwise, and that diagnosis has implications beyond OTC blockade. A luteal-phase mood crash that includes intrusive thoughts about self-harm is a PMDD presentation that deserves a real workup and is not safely treated with antihistamine self-prescribing. Severe depression of any cycle pattern deserves psychiatric care.
If you have been on the stack for three months and the symptoms have not budged, the histamine angle is probably not your lever and continuing is unlikely to change that. If the symptoms came back when you stopped, that is real information, and a clinician who knows this literature can help you think about what to do with it. If you are a candidate for HRT and have been avoiding it because of post-WHI fear or cost, the 2025 Menopause Society guidelines and an honest conversation with a menopause-trained clinician is the conversation that actually matters for your healthspan.
What this means for the woman in front of me: the right answer is almost never "Pepcid plus Claritin or nothing." It is "here is the framework, here is the screen, here are the questions, and here is who to ask."
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
Frequently Asked Questions
Is Pepcid plus Claritin safe to take long-term for perimenopause?
Short-term use in healthy adults is well-tolerated. Long-term concerns are vitamin B12 and iron malabsorption with chronic famotidine, drug interactions with tizanidine and pH-dependent medications, and masking of conditions that warrant evaluation. If you run the stack for more than a few months, annual B12, ferritin, and CBC labs are reasonable to track.
Will antihistamines interfere with my HRT?
Direct pharmacokinetic interference is not a major concern. The more interesting interaction is biological. Estradiol activates mast cells, and oral micronized progesterone stabilizes them. For a woman with histamine-pattern symptoms on HRT, getting the progesterone right is often where the conversation needs to happen, not stopping the estradiol.
Which antihistamine is best, Allegra, Claritin, or Zyrtec?
All three are second-generation H1 blockers with low anticholinergic burden. Fexofenadine (Allegra) and loratadine (Claritin) are non-sedating for most people. Cetirizine (Zyrtec) can be mildly sedating. Lactation data is most reassuring for loratadine and fexofenadine. There is no head-to-head trial in perimenopausal women to declare a winner.
Do I need both Pepcid and Claritin or just one?
The trend uses both because H1 and H2 receptors cover different symptom territory. H1 blockers help itch, hives, and flushing. H2 blockers act on stomach parietal cells and have been studied for cognitive symptoms in adjacent populations. Some women report response to one alone. The combination has not been formally tested in perimenopausal women.
Will this raise my dementia risk?
The clear dementia signal is for first-generation antihistamines like diphenhydramine (Benadryl) and doxylamine (Unisom) due to anticholinergic burden, per the Gray 2015 cohort study. Second-generation H1 antihistamines and famotidine have mixed and largely reassuring data. The bigger concern is reaching for first-gen agents for sleep on top of the daily stack.
Does this mean I have histamine intolerance or MCAS?
No. Response to a receptor blocker is not a diagnosis. Mast cell activation syndrome has formal multi-organ criteria with objective lab confirmation. Histamine intolerance has no validated biomarker and DAO testing is not reliable as a standalone test. Symptom relief on antihistamines is information, not a label.
References
Gray, S. L., et al. (2015). Cumulative use of strong anticholinergics and incident dementia: A prospective cohort study. JAMA Internal Medicine, 175(3), 401-407. PMID 25621434. https://pubmed.ncbi.nlm.nih.gov/25621434/
Hrubisko, M., Danis, R., Huorka, M., and Hrubiskova, K. (2020). Histamine intolerance: The current state of the art. Biomolecules, 11(8), 1262. PMC7463562. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7463562/
Jensen, F., et al. (2010). Estradiol and progesterone regulate the migration of mast cells from the periphery to the uterus and induce their maturation and degranulation. PLOS One, 5(12), e14409. https://doi.org/10.1371/journal.pone.0014409
Kalogeromitros, D., et al. (1976). Histamine metabolism and female sex hormones in women. Annals of Internal Medicine. PMID 998172. https://pubmed.ncbi.nlm.nih.gov/998172/
Lederman, S., et al. (2023). Fezolinetant for treatment of moderate-to-severe vasomotor symptoms associated with menopause (SKYLIGHT 1): A phase 3 randomised controlled study. The Lancet, 401(10382), 1091-1102. PMID 36924778. https://pubmed.ncbi.nlm.nih.gov/36924778/
Liu, J., et al. (2023). Magnitude of placebo response in clinical trials of paroxetine for vasomotor symptoms: A meta-analysis. Frontiers in Psychiatry, 14, 1204163. https://doi.org/10.3389/fpsyt.2023.1204163
Momtazmanesh, S., et al. (2023). Effect of famotidine on cognitive and behavioral dysfunctions induced in post-COVID-19 infection: A randomized, double-blind, and placebo-controlled study. Brain and Behavior, 13(8), e3091. PMID 37327698. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10229204/
Pan, Y., et al. (2020). Open-label placebos for menopausal hot flushes: A randomized controlled trial. Scientific Reports, 10, 20090.
Rance, N. E., et al. (2013). Modulation of body temperature and LH secretion by hypothalamic KNDy neurons: A novel hypothesis on the mechanism of hot flushes. Frontiers in Neuroendocrinology, 34(3), 211-227. PMC3833827. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3833827/
Russek, L., et al. (2023). Treatment and maintenance of interstitial cystitis/bladder pain syndrome in female patients with cetirizine-famotidine: A case series. Case Reports in Clinical Medicine.
Sherman, S., et al. (2014). Placebo improvement in pharmacologic treatment of menopausal hot flashes: Time course, duration, and predictors. Menopause, 21(11), 1136-1144. PMC4333078. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4333078/
Sussman, G., et al. (2021). Evaluation of pharmacologic treatments for H1 antihistamine-refractory chronic spontaneous urticaria: A systematic review and network meta-analysis. JAMA Dermatology. PMID 34431983. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8387945/
The Menopause Society. (2025). The 2025 menopausal hormone therapy guidelines. PMC12438153. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12438153/
Vasiadi, M., et al. (2006). Progesterone inhibits mast cell secretion. International Journal of Immunopathology and Pharmacology, 19(4), 787-794. PMID 17166400. https://pubmed.ncbi.nlm.nih.gov/17166400/
Zaitsu, M., et al. (2007). Estradiol activates mast cells via a non-genomic estrogen receptor-alpha and calcium influx. Molecular Immunology, 44(8), 1977-1985. PMID 17084457. https://pubmed.ncbi.nlm.nih.gov/17084457/
Zhou, J., et al. (2019). The combination of loratadine with famotidine to relieve the symptoms of urinary frequency in female patients with bladder function disorders: First report of three cases. Journal of Clinical Pharmacy and Therapeutics, 44(4), 643-646.
Frontiers in Allergy. (2024). Sex hormones and allergies: Exploring the gender differences in immune responses. Frontiers in Allergy, 5, 1483919. https://doi.org/10.3389/falgy.2024.1483919
Drugs and Lactation Database (LactMed). Famotidine (NBK501267), Loratadine (NBK501009), Cetirizine (NBK501509), Fexofenadine (NBK500677). https://www.ncbi.nlm.nih.gov/books/NBK501922/