Your Hormone Symptoms May Be a Gut Problem First
If your hormone labs came back normal but you still feel off, you are not imagining it. You are also not one supplement away from fixed. Here is the honest version. Your gut and your estrogen genuinely talk to each other, yet no human trial proves that fixing your gut will fix your hormones.
That sentence is the whole article in one breath, and I want you to have it before anything else. I am Dr. Shad Abdulla, ND, a naturopathic doctor who reads the actual studies instead of the supplement labels. Below, I will walk you through what conventional medicine misses here and what the gut-hormone loop actually is. Then I will show you which moves are worth doing this week, and which tests and pills are worth skipping.
Why does your doctor say your labs are normal when you feel terrible?
Your labs can sit perfectly in range while your body still struggles. A number in range is not the same as a system working well. Conventional medicine runs your hormone panel, sees it land in the reference window, and tells you nothing is wrong. That is where the gap opens.
I hear a version of this constantly. A woman did the work. She cleaned up her diet, she started moving, maybe she even started hormone therapy, and she still feels bloated, tired, and dismissed.
The load-bearing word in how women describe this is “still.” Still bloated. Still exhausted. Still being sent home.
Here is what conventional medicine misses here. It treats your gut and your hormones as two separate departments that never speak.
The naturopathic lens on this is different. It asks a root-cause question instead of a single-organ question. What upstream system might be shaping how you feel, even when each individual number looks fine?
That root-cause version of the question points at the gut. Not because the gut is a magic switch, but because the gut and your hormones share machinery that a standard panel never measures. In cases I’ve reviewed, the most relieved women are not the ones handed a new pill. They are the ones who finally hear that their experience has a mechanism.
The takeaway: a “normal” lab measures the hormone in your blood right now. It does not measure how your gut recycles that hormone or how much low-grade inflammation your gut barrier is letting through. Ask your doctor what your symptoms might mean beyond the single in-range number.
What is the gut-hormone connection, in plain language?
The gut-hormone connection means your gut bacteria can change how much estrogen stays in your body, and how much background inflammation you carry. Two mechanisms drive this. Both are real biology. Both are still mostly proven in mice, which matters and I will not hide it.
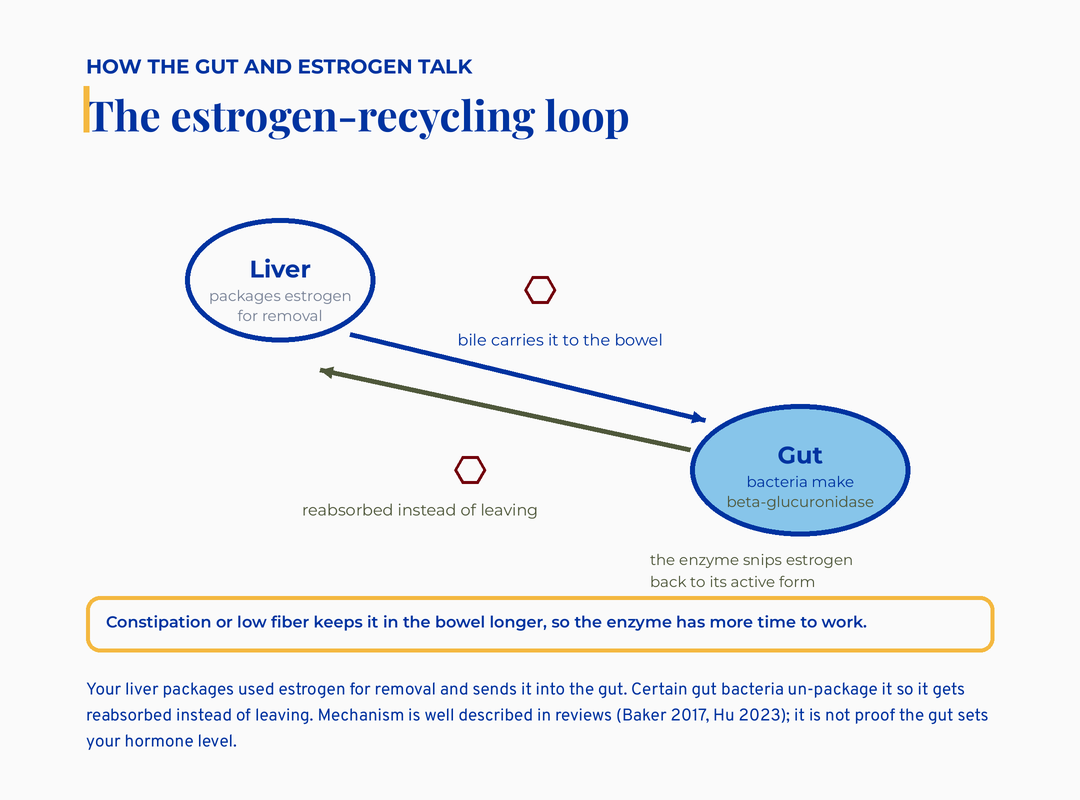
The estrogen-recycling loop: the liver packages estrogen into bile to the gut, where bacterial beta-glucuronidase reactivates it so it is reabsorbed instead of leaving
The first mechanism is the estrobolome. The estrobolome is the set of gut bacteria that act on estrogen, nothing more exotic than that. Your liver packages used estrogen for removal and sends it into your gut to leave the body.
Certain gut bacteria make an enzyme called beta-glucuronidase. Beta-glucuronidase is a molecular scissors that snips estrogen back into its active form. So instead of leaving, it gets reabsorbed.
That reabsorption loop has a name worth knowing: enterohepatic recirculation. Enterohepatic recirculation simply means a substance travels liver to gut and back to blood, in a loop, rather than straight out. When you are constipated or low on fiber, packaged estrogen sits in your bowel longer, and the bacterial scissors have more time to work.
Across 28 studies, women with PCOS showed lower gut diversity than women without it (Li 2023, n=1,022). I want to be careful with that number. It is a pattern, not a proven cause, and it is partly tangled up with body weight. PCOS, by the way, means polycystic ovary syndrome, a common hormonal and metabolic condition.
The honest read is that a less diverse, more inflammation-leaning gut tends to travel alongside this hormonal picture. It does not mean one clearly causes the other.
If you want the perimenopause-specific version of this loop, I went deeper in the estrogen, gut, and vascular axis in perimenopause. There the same recycling machinery interacts with declining estrogen. That piece is the close companion to this one for women in their early forties.
The takeaway: the estrobolome is real, and it is just “the gut bacteria that act on your estrogen.” Higher fiber and regular bowel movements give those bacteria less time to recycle estrogen. That is a lever you control, today, without a single supplement.
Could a leaky gut be feeding your hormone and metabolic symptoms?
A leaky gut barrier can let bacterial fragments slip into your bloodstream. Those fragments can stir up low-grade inflammation that amplifies how rough you feel. This is the second mechanism, and almost nobody translates it for you, so let me.
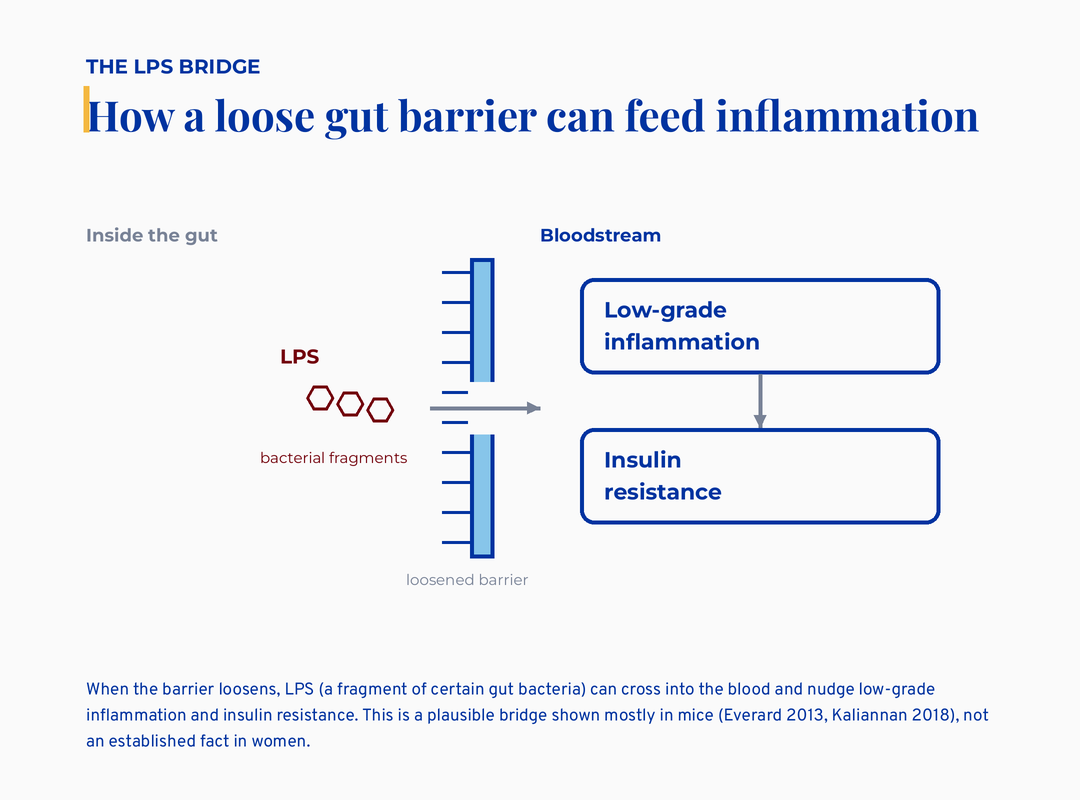
The LPS bridge: when the gut barrier loosens, LPS bacterial fragments cross into the bloodstream and nudge low-grade inflammation and insulin resistance, shown mostly in mice
Your gut lining is supposed to be a tight wall. When that wall loosens, pieces of bacteria called LPS leak through. LPS stands for lipopolysaccharide, which is just a fragment of the outer coat of certain gut bacteria. Your immune system reads loose LPS as a threat and switches on a slow, simmering inflammation.
That simmer has a clinical name: metabolic endotoxemia. Metabolic endotoxemia means a low, chronic level of those bacterial fragments in your blood. It is enough to nudge inflammation and insulin resistance without ever making you acutely sick. Insulin resistance, in plain terms, is your body needing more and more insulin to do the same blood-sugar job.
Here is the honest tier on this. The cleanest proof that lowering this fragment load reverses the inflammation comes from mouse studies, not from women like you. One large analysis of synbiotic supplements in people did not move the inflammation markers at all.
So I hold it loosely. This is a plausible bridge between gut trouble and how you feel, not an established fact.
The naturopathic frame still finds it useful. It explains the “I feel inflamed and puffy and foggy and my labs are fine” experience that the hormone panel ignores. My clinical-nutrition training keeps pulling me back to the same unglamorous answer.
What this means for the woman in front of me is simple. The fix is not a fancy test. The fix is the boring, low-risk work of feeding the gut barrier well.
The takeaway: “leaky gut” here means a loosened barrier letting bacterial fragments through, and that can feed background inflammation. You cannot reliably measure this at home yet, so do not pay for a test that claims to. Spend that money on fiber and sleep instead.
Does fixing your gut actually fix your hormones?
No, the evidence does not yet support that, and I would rather tell you the truth than sell you a clean story. In 1,000 women, gut estrogen-recycling genes showed no difference in an estrogen-driven disease (Saare 2024). That is the single largest study of this question, and it came up empty.
Sit with what that means. The wellness version says your estrobolome is broken, so fix your gut and your hormones will follow. The largest dataset we have did not find the estrogen-recycling difference that story depends on.
And a separate measurement found that the beta-glucuronidase enzyme on its own did not track with active estrogen in stool. The single-enzyme story is too simple.
I am not telling you the gut does not matter. I am telling you the loop runs both ways, and the human outcome data is thin.
Estrogen shapes the gut, and the gut shapes estrogen. No trial in women aged 30 to 45 has shown that gut-targeted therapy resolves hormonal symptoms. That is a gap in the science, not a flaw in you.
There is one bright spot worth naming honestly. A 6-month synbiotic cut testosterone 40% versus 5% on placebo, independent of weight loss (Chudzicka-Strugala 2024). A synbiotic is just a probiotic plus the fiber that feeds it. That is a single trial in PCOS, flagged as needing standalone confirmation, so I name it as one promising study, never as “studies show.”
And if you do choose a probiotic, the strain on the label matters more than the brand on the front. I broke down why most products miss in why your probiotic isn’t working. The short version is that “probiotic” on a label tells you almost nothing without a named, studied strain.
This is the root-cause version of the question done honestly. The root cause is not “your gut is broken, here is the test.” It is a real two-way loop.
The low-risk gut basics are worth doing while the big evidence catches up. The overpriced tests and pills are worth skipping.
The takeaway: “heal your gut and your hormones will follow” is not proven in women your age. Be skeptical of any product that promises it. The honest move is to do the safe gut basics for their own sake, not as a guaranteed hormone cure.
If the gut loop is thin, what does have real evidence here?
Plenty, and I want to be generous here, because the honest skepticism above can leave you thinking nothing works, and that is not true. Most of the real evidence lives on the metabolic side of this axis, the insulin-and-androgen part rather than the estrogen-recycling part. Here are the options with actual trials, tier-labeled. None of this is a prescription. It is education to take to your own clinician.
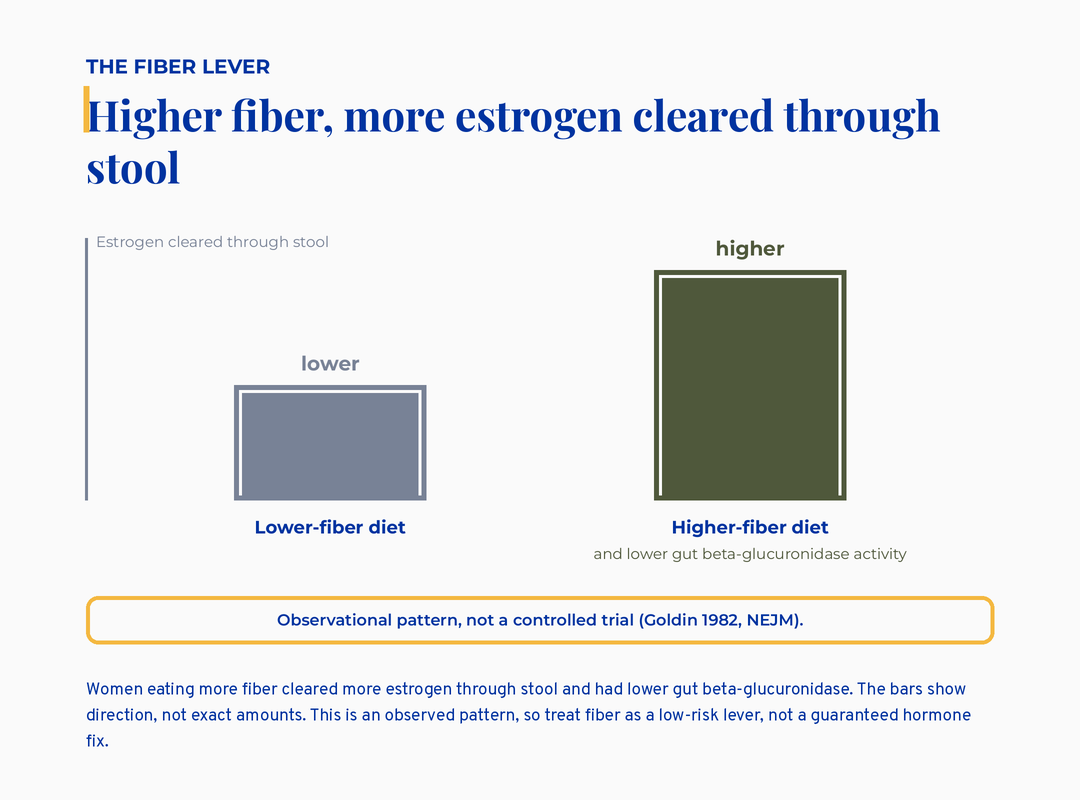
Bar comparison: a higher-fiber diet clears more estrogen through stool than a lower-fiber diet, an observed pattern not a controlled trial
Inositol has the strongest evidence of anything on this page. Inositol is a sugar-like compound your cells use for insulin signaling. An umbrella review pooling 28 separate meta-analyses found it improved fasting insulin, and in women with PCOS trying to conceive it raised ovulation rates (Moslehi 2023). A network analysis of 22 trials found myo-inositol combined with D-chiro-inositol actually outperformed metformin for restoring regular cycles and lowered both testosterone and insulin resistance (Zhao 2021). If your “off” is really an insulin-and-cycle story, this is the best-supported lever here, and almost nobody in the gut-hormone conversation names it.
Flaxseed is the first supplement on the PCOS protocol I trained with, and the trials back it. Two tablespoons of ground flax a day is fiber plus lignans, plant compounds that interact with estrogen, so it touches both sides of this loop. In a double-blind trial, flaxseed oil lowered insulin, insulin resistance, a hair-growth score tied to high androgens, triglycerides, and an inflammation marker (Mirmasoumi 2017). A separate trial found milled flaxseed improved the FSH-to-LH balance that is often off in PCOS (Najdgholami 2025). It is cheap, it is food, and it carries the same fiber benefit this whole article is built on.
Berberine deserves an honest hearing, not just a warning. I flag berberine’s real cautions on the card below, and I stand by them. But it is not fair to name a plant compound only by its risks. Berberine is a bright-yellow alkaloid from plants like goldenseal and barberry, and across PCOS trials it improves insulin resistance, landing alongside metformin and inositol as a genuine insulin sensitizer (Zhao 2021). The honest full picture holds both things at once: real metabolic evidence, and real cautions. It interacts with several medications through the liver’s drug-processing enzymes, and it is off the table if you are pregnant, breastfeeding, or trying to conceive, because it crosses the placenta and into milk. So it is a supervised option for the right woman, never a casual one.
A traditional note, named honestly. Chaste tree, or Vitex, is a botanical I trained on as a hormone modulator, used for a long time for irregular or difficult cycles and PMS. Its evidence is mixed, and it works on the cycle side, not the gut or the insulin side, so I name it as tradition with modest support rather than a metabolic fix. It is also not for everyone. Avoid it in pregnancy and alongside hormonal birth control.
The takeaway: honest skepticism about gut-and-estrogen does not mean nothing helps. On the metabolic side, inositol has the strongest evidence, flaxseed is food-first and well-supported, and berberine carries real metabolic data alongside real cautions. These are clinician conversations, not self-prescriptions.
Is estrogen dominance a diagnosis you can give yourself?
No, estrogen dominance is not something you can self-diagnose from symptoms, and most women using the term have never measured their estrogen. I say this with zero judgment, because the label fills a real vacuum. Your workup came back normal and nobody explained anything, so a name that fits feels like relief.
Here is the catch that the marketing skips. Many women who call themselves “estrogen dominant” may actually be running low estrogen, not high, especially heading into perimenopause where estrogen swings hard and unpredictably. Estrogen status alone does not even predict your gut microbiome, based on a 2026 review pooling several studies. So a symptom checklist cannot tell you which direction your estrogen is going.
This is why the popular advice to “lower your estrobolome” worries me. Whether you want more or less of that estrogen-recycling activity depends entirely on your life stage. In your reproductive years with an estrogen-excess pattern, slowing reabsorption might help. In menopause, that same enzyme activity raises estrogen, which is the thing menopausal women are trying to get back.
So the same supplement aimed at the same enzyme can point in opposite directions for two different women. DIM is the clearest example. DIM, a compound from cruciferous vegetables, may reduce estrogen’s effect, which is unwanted if you are menopausal and want that estrogen. Blanket “clear your excess estrogen” advice ignores all of this.
This is also where PCOS and thyroid symptoms blur together, since both can drive the “labs normal but I feel off” experience. I sorted out which labs actually matter in the PCOS and thyroid panel breakdown. The wrong self-diagnosis sends you toward the wrong fix. Measurement beats a symptom checklist every time.
The takeaway: do not self-diagnose estrogen dominance from a symptom list. If your estrogen genuinely matters to your care, ask for actual measurement and life-stage context. A label you gave yourself can send you toward the wrong supplement.
What about birth control, antibiotics, and PPIs from years ago?
Past medications can genuinely shift your gut for a long time, and it is reasonable to wonder whether they set this in motion. Antibiotics reduce bacterial diversity, and that diversity does not always bounce all the way back. Birth control and acid-blocking PPIs also change the gut environment. PPI, here, means proton pump inhibitor, a common heartburn drug that lowers stomach acid.
So the instinct that “something years ago changed my gut” is not paranoid. It is biologically plausible.
What I want to protect you from is the next leap. That is the one that calls a single past exposure the proven root cause of everything you feel now. We do not have the data to draw that straight line, and a story that tidy usually has a product attached.
The useful move is forward-looking, not backward-blaming. You cannot undo a course of antibiotics from 2015. You can feed gut diversity now with fiber variety, fermented foods, and regular bowel habits. Those rebuild the same diversity those drugs depleted, and they cost almost nothing.
In clinical settings I’ve worked in, this reframe lands as relief rather than blame. The point is not to find the one villain in your history. The point is to give the gut what it needs going forward, while staying honest that we cannot prove which past exposure mattered most.
The takeaway: old antibiotics, the pill, and PPIs can plausibly shift gut diversity. You still cannot pin all of today’s symptoms on one of them with certainty. Focus on rebuilding diversity now. Diet variety is the most evidence-friendly lever you have.
What I’d do this week
Here is the part you can actually act on, and I built it to be honest about which moves are proven and which are oversold. This is the one place I am giving you a full reference card. Save it for your next bloodwork appointment.
This card is education, not a treatment plan. The loop between gut and hormones runs both ways, and the human data is associative. No trial yet shows that fixing the gut resolves hormonal symptoms in women 30 to 45.
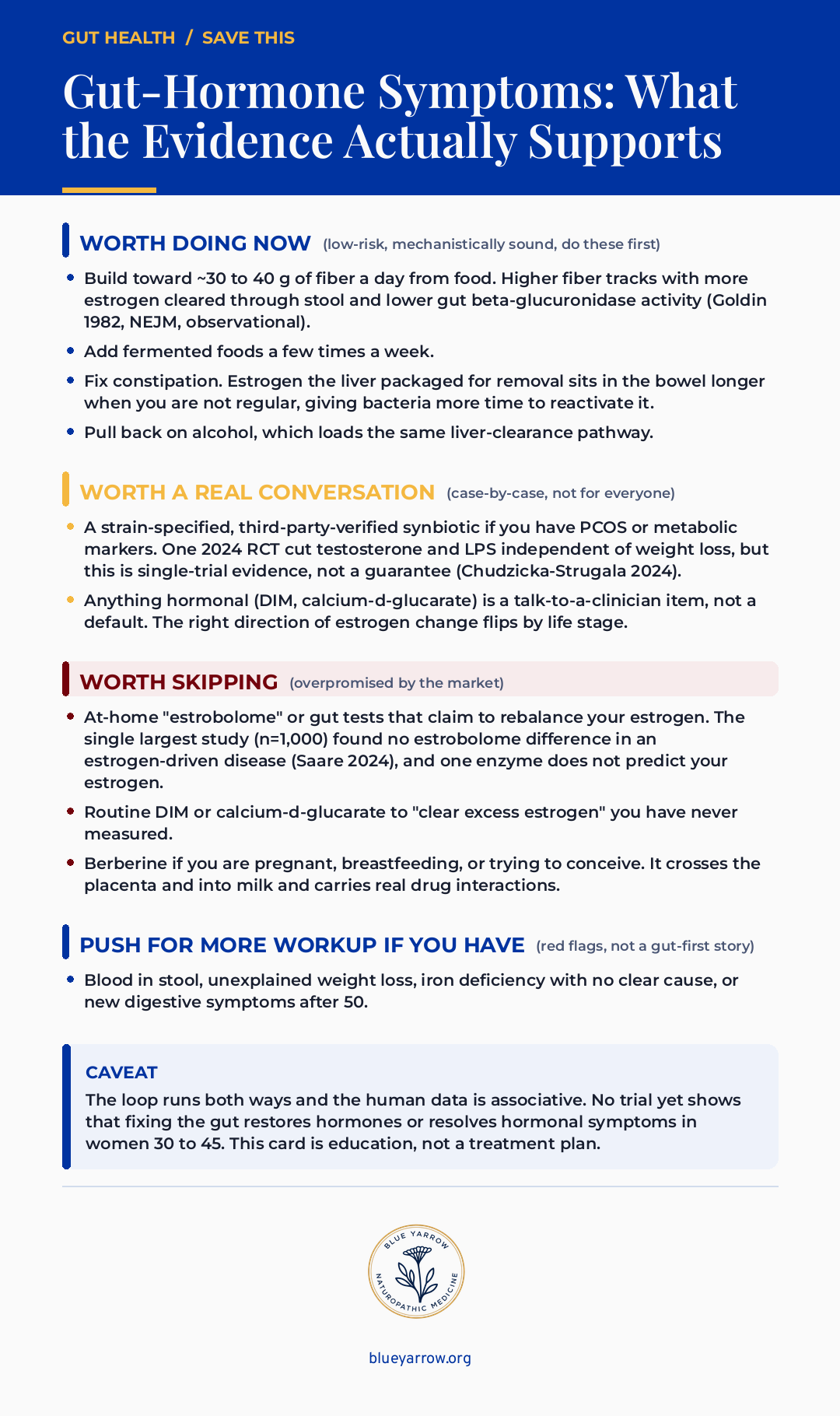
If you do only one thing this week, fix the constipation and push the fiber. That single move touches the estrogen-recycling loop directly, it is free, and it carries no real downside.
When is it time to push for more, not more supplements?
Some symptoms are not a gut-hormone puzzle to optimize, they are a reason to get seen promptly. I never want a calm “it’s probably your gut” message to talk you out of a workup you actually need. So I will name the lines plainly.
Push your doctor for more investigation if you notice certain warning signs. Those are blood in your stool, unexplained weight loss, iron deficiency with no clear cause, or new digestive symptoms after age 50. These do not fit the “labs normal, feel off” story, and they are not things to manage with fiber and fermented foods alone.
What this means for the woman reading this is a boundary worth holding. The honest gut-hormone conversation is for the woman whose serious workup is clean and who is still left without answers. It is not a replacement for that workup. If anything on that red-flag list is true for you, that comes first.
The takeaway: know the four red flags, because they override everything else on this page. Blood in stool, unexplained weight loss, unexplained iron deficiency, or new symptoms after 50 mean you ask for a workup, not a supplement.
Frequently asked questions
Is this hormones or my gut? Most likely it is both, feeding each other, which is why an either-or framing stalls you. Your gut influences how estrogen recirculates, and your estrogen shapes your gut in return. The loop runs both ways. Start with the low-risk gut basics, since they help regardless of which side started it.
My bloodwork is clear, so why do I feel like this? A normal lab measures the hormone in your blood at one moment. It does not measure how your gut recycles estrogen or how much low-grade inflammation your gut barrier lets through. Clear labs and real symptoms can coexist. Your experience is data too, even when the panel looks fine.
Could antibiotics, birth control, or PPIs have caused this? Plausibly, yes, in part. Antibiotics reduce gut diversity that does not always rebound, and birth control and PPIs shift the gut environment too. But you cannot pin all of today’s symptoms on one past exposure with certainty. Rebuilding diversity now matters more than naming the original culprit.
Does HRT help gut symptoms or make bloating worse? It varies by woman, and honestly the data here is thin. Estrogen influences gut motility and the gut barrier, so hormone therapy can shift digestion in either direction. Some women notice easier digestion, some notice more bloating early on. Track your own response rather than expecting one universal answer.
Should I take DIM or calcium-d-glucarate to clear estrogen? Not as a default, and not from a self-diagnosis. The human estrogen-outcome trials are tiny or absent, and the right direction of estrogen change depends on your life stage. DIM may even blunt hormone therapy. These belong in a clinician conversation, especially if you could become pregnant.
If gut-and-hormone supplements are oversold, is there anything that actually works? Yes, mostly on the metabolic side. Inositol has the strongest evidence here: pooled analyses show it improves insulin resistance and ovulation in PCOS, rivaling metformin for cycle regularity (Moslehi 2023; Zhao 2021). Ground flaxseed is food-first and well-supported, improving insulin resistance and the FSH-to-LH balance (Mirmasoumi 2017; Najdgholami 2025). Berberine has real metabolic data in PCOS but also real drug interactions and is off-limits in pregnancy, lactation, or when trying to conceive. These are clinician conversations, not self-prescriptions.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Li, P., El-Omar, E. M., Wan, Z., et al. (2023). Perturbations in gut microbiota composition in patients with PCOS: A systematic review and meta-analysis. BMC Medicine, 21. https://doi.org/10.1186/s12916-023-02975-8
2. Salliss, M. E., Saare, M., et al. (2024). Gut microbiome in endometriosis: A cohort study on 1000 individuals. BMC Medicine, 22. https://doi.org/10.1186/s12916-024-03503-y
3. Chudzicka-Strugala, I., Kubiak, A., Banaszewska, B., et al. (2024). Synbiotic supplementation in overweight/obese PCOS. Archives of Gynecology and Obstetrics. https://doi.org/10.1007/s00404-024-07833-3
4. Saravinovska, K., Santi, D., Marina, L. V., et al. (2026). The impact of estrogen status on the gut microbiome: A systematic review and meta-analysis. Frontiers in Endocrinology. https://doi.org/10.3389/fendo.2026.1780806
5. Baker, J. M., Al-Nakkash, L., & Herbst-Kralovetz, M. M. (2017). Estrogen-gut microbiome axis: Physiological and clinical implications. Maturitas, 103, 45-53. https://doi.org/10.1016/j.maturitas.2017.06.025
6. Hu, S., Ding, Q., Zhang, W., et al. (2023). Gut microbial beta-glucuronidase: A vital regulator in female estrogen metabolism. Gut Microbes, 15(1). https://doi.org/10.1080/19490976.2023.2236749
7. Everard, A., Belzer, C., Cani, P. D., et al. (2013). Cross-talk between Akkermansia muciniphila and intestinal epithelium controls diet-induced obesity. PNAS, 110(22). https://doi.org/10.1073/pnas.1219451110
8. Goldin, B. R., Gorbach, S. L., et al. (1982). Estrogen excretion patterns and plasma levels in vegetarian and omnivorous women. NEJM, 307(25). https://doi.org/10.1056/NEJM198212163072502
9. Newman, M., et al. (2025). DIM and urinary estrogen profiles in women on transdermal estradiol. Menopause. https://doi.org/10.1097/GME.0000000000002542
10. Moslehi, N., Zeraattalab-Motlagh, S., Rahimi Sakak, F., et al. (2023). Effects of nutrition on metabolic and endocrine outcomes in women with polycystic ovary syndrome: An umbrella review of meta-analyses of randomized controlled trials. Nutrition Reviews, 81(5), 555-577. https://doi.org/10.1093/nutrit/nuac075
11. Zhao, H., Xing, C., Zhang, J., & He, B. (2021). Comparative efficacy of oral insulin sensitizers metformin, thiazolidinediones, inositol, and berberine in improving endocrine and metabolic profiles in women with PCOS: A network meta-analysis. Reproductive Health, 18(1), 171. https://doi.org/10.1186/s12978-021-01207-7
12. Mirmasoumi, G., Fazilati, M., Foroozanfard, F., et al. (2017). The effects of flaxseed oil omega-3 fatty acids supplementation on metabolic status of patients with polycystic ovary syndrome: A randomized, double-blind, placebo-controlled trial. Experimental and Clinical Endocrinology & Diabetes, 126(4), 222-228. https://doi.org/10.1055/s-0043-119751
13. Najdgholami, Z., Sedgi, F. M., Ghalishourani, S. S., et al. (2025). Flaxseed intervention and reproductive endocrine profiles in patients with polycystic ovary syndrome: An open-labeled randomized controlled clinical trial. Frontiers in Endocrinology, 16, 1531762. https://doi.org/10.3389/fendo.2025.1531762
14. SUHS / Sonoran University naturopathic clinical training, PCOS treatment protocol and Hormone Modulator Herbs reference (Dr. Shad Abdulla, ND). [Naturopathic clinical training: flaxseed for insulin resistance, higher-protein lower-glycemic pattern, and chaste tree/Vitex as a hormone-modulating botanical.]