Rebuilding Your Gut After Antibiotics: What the Data Says
You finished the antibiotics or the herbal antimicrobials, you did everything you were told, and it came back. So now what? Here is the plain answer most rebuild content never gives you. The kill phase is only half the job, and most of the rebuild you were sold is mechanism and tradition, not proof. The part that actually holds is motility and finding the root cause. Your relapse is not a personal failure. You were handed half a treatment. What follows is the honest, evidence-tiered version of the repair phase: what each step is for, how strong the data behind it really is, and where the science simply has not caught up.
Why does SIBO keep coming back after antibiotics?
SIBO returns in close to half of patients within nine months of one antibiotic course (Lauritano 2008). That single number reframes everything. If you treated it once and it came back, you are not the exception. You are the rule the marketing leaves out.
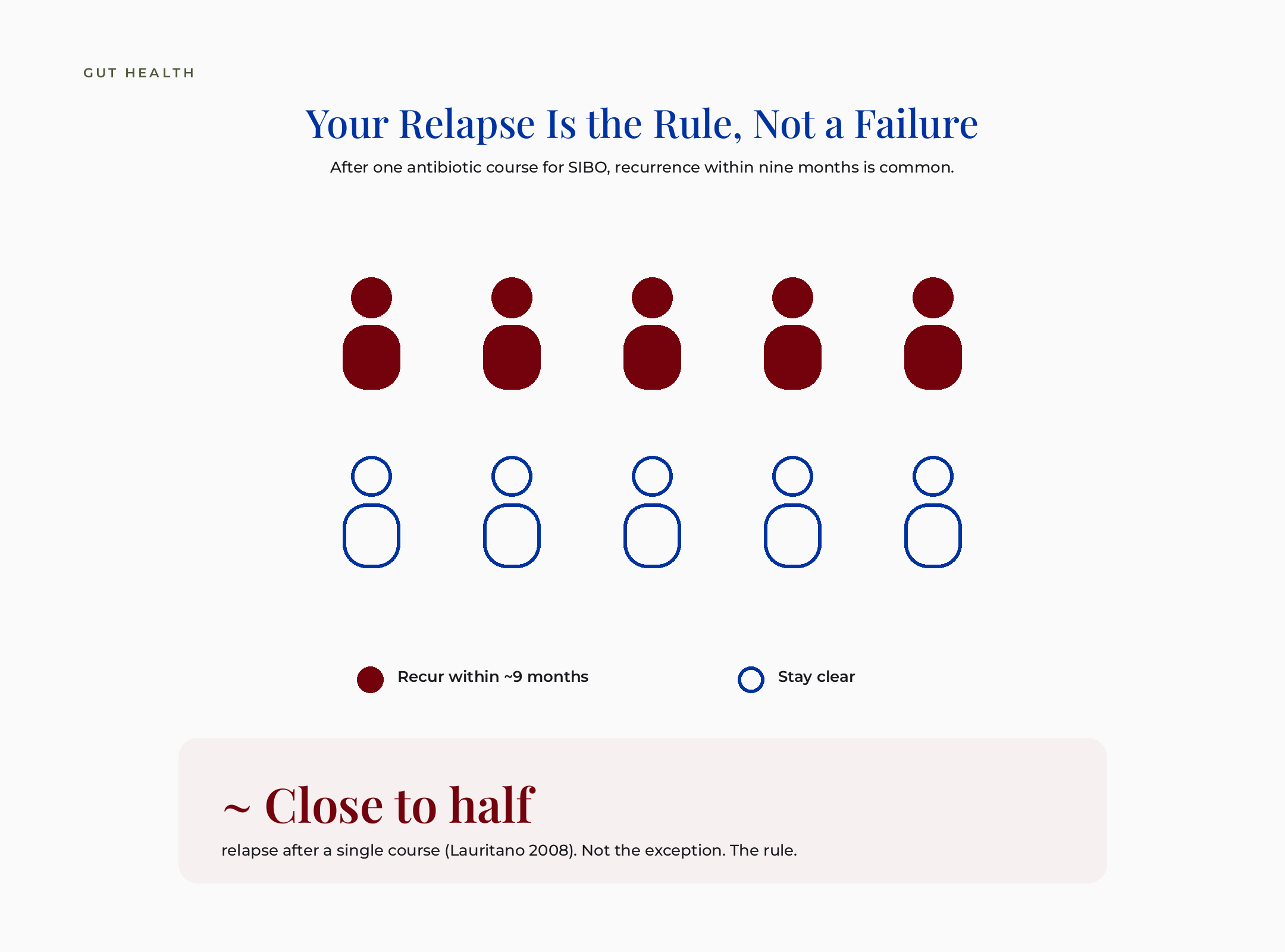
Pictograph showing close to half of patients relapse within about nine months of one antibiotic course for SIBO
Let me back up and name the thing plainly. SIBO means small intestinal bacterial overgrowth, meaning bacteria that should live in the apartment downstairs, your large intestine, set up shop on your second floor, the small intestine where they do not belong. Antibiotics or herbal antimicrobials clear the overgrowth. On the herbal side, the ones I trained on are berberine, allicin from garlic (the usual pick when methane runs high), oregano oil, neem, and uva ursi. They are real kill-phase tools, and each deserves its own piece, so here I will keep it short and just name them, with one safety line that matters: berberine and neem are off-limits in pregnancy, while breastfeeding, and when trying to conceive. None of them, herb or antibiotic, change why the bacteria moved upstairs in the first place. That is the gap. The kill phase is well defined and easy to sell. The reason it relapses is neither.
What this means for the woman in front of me: if your gut symptoms returned a few weeks or months after a successful round, that is a known pattern, not a sign you failed the treatment. The honest read is that you were given the first half of a two-part job and sent home.
This is the next piece in my SIBO series. If you followed the relapse and subtypes piece, you already know recurrence is the rule. Here I want to go further into what the repair phase actually involves, and where the evidence is strong, thin, or borrowed.
For the why-it-relapses groundwork, I wrote a full piece on SIBO subtypes and why it keeps relapsing. This article picks up where that one ends.
What does conventional medicine miss about post-antibiotic gut repair?
What conventional medicine misses here is not the relapse rate. Gastroenterologists know SIBO recurs, and the major guidelines say so directly. What gets lost in a short appointment is the answer to your actual question: now what? The guideline answer exists, but it is rarely handed to you in a usable form.
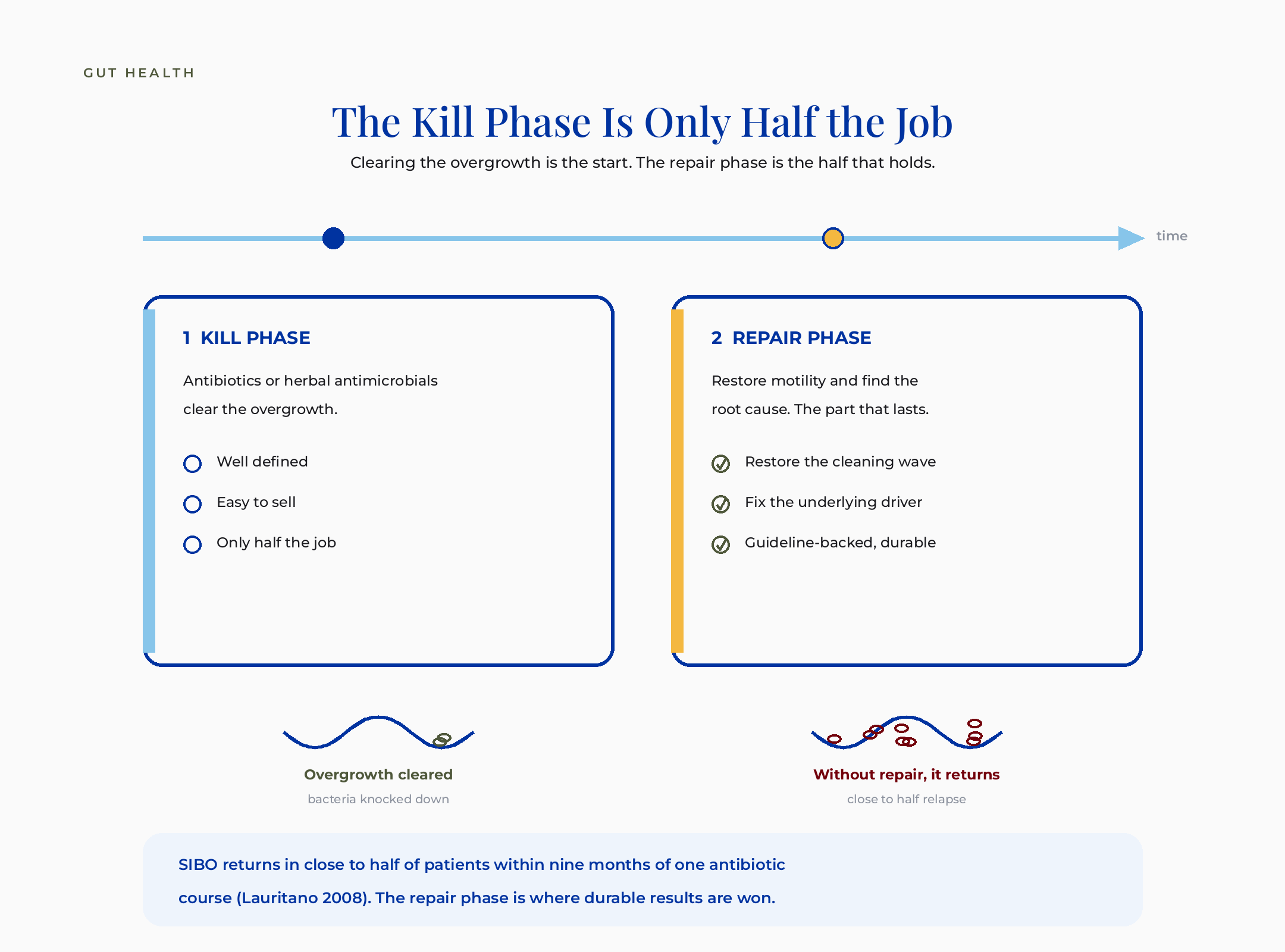
Two-phase timeline: the kill phase clears the overgrowth, the repair phase restores motility and the root cause, where durable results are won
Here is the third position, the one that sits between the two stories you have been told. Conventional gastroenterology treats the overgrowth with antibiotics, agrees relapse is common, and says the durable fix is correcting the underlying cause. The wellness industry says kill it, then rebuild and reseed with a glutamine and probiotic stack. The honest version takes the best of both. The kill phase is real and necessary. The root-cause work is the part that lasts. And a good chunk of the rebuild stack is mechanism and tradition dressed up as proof.
The naturopathic lens on this is not “more supplements.” Done well, it is the opposite. It is the discipline of asking why the terrain let bacteria overgrow in the first place, then being honest about which repair steps have evidence and which are hope. That is the root-cause version of the question, and it is the part no supplement funnel leads with, because it is the least marketable.
Bolded micro-summary: the durable work is restoring motility and finding the root cause. Most of the branded “rebuild” stack is supporting biology that is real, with evidence that is thinner than the confidence used to sell it.
What actually causes SIBO to relapse? The root cause, not the bacteria
The most durable approach to recurrence is finding and correcting what caused the overgrowth in the first place. That is the one thing the gastroenterology guidelines actually agree on (ACG 2020, AGA 2020). It is also the least exciting sentence in this whole article, which is exactly why it does not sell.
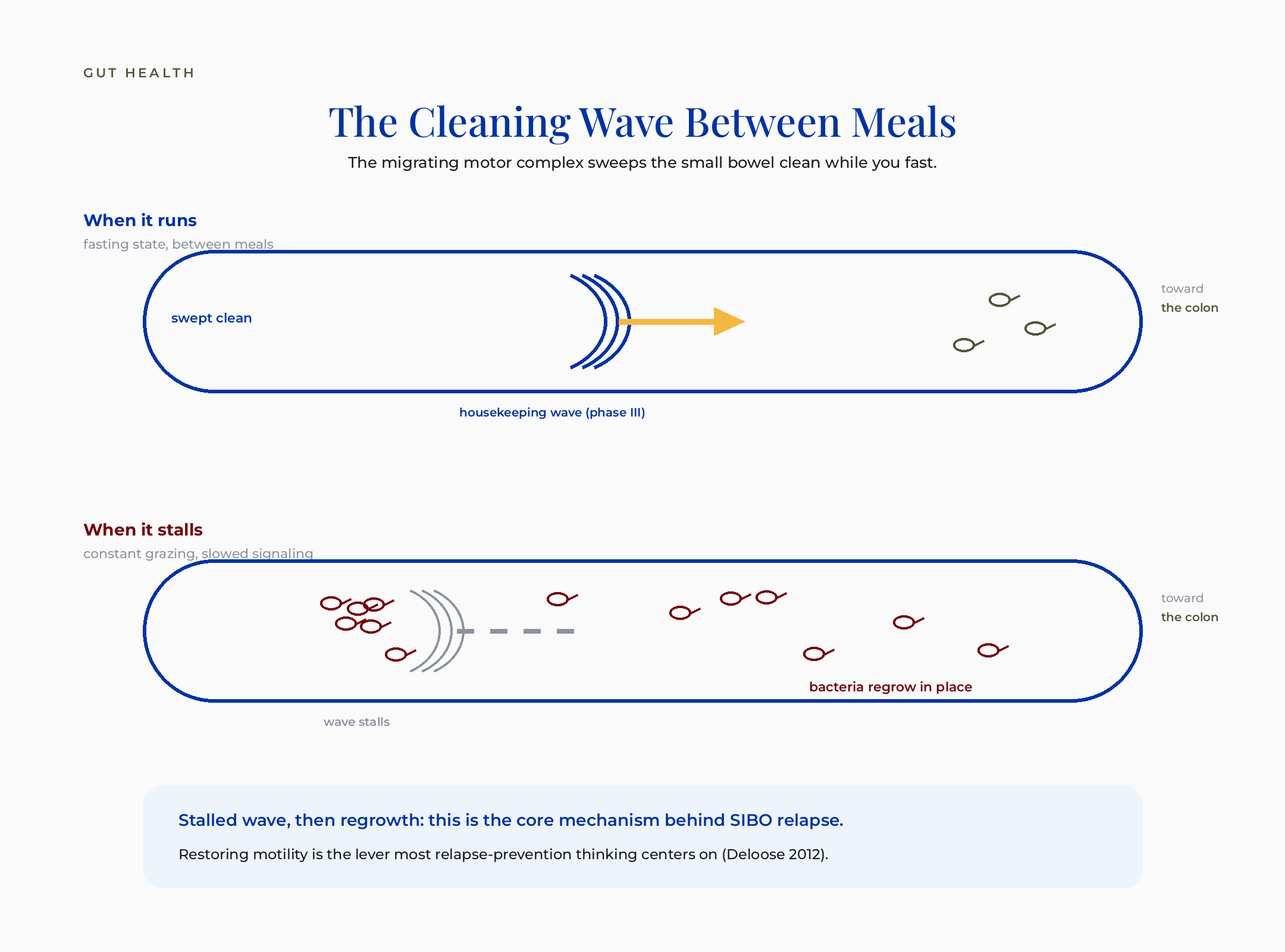
The migrating motor complex: between meals a housekeeping wave sweeps the small bowel clean, and when it stalls bacteria regrow in place, the core mechanism behind SIBO relapse
So what are the underlying drivers? Slow motility. Anatomy, like adhesions or a structural narrowing. Low stomach acid. Certain medications that slow the gut. The bacteria that grew were a symptom. The reason they could grow is the actual target. Clear the bacteria without changing the terrain and you have reset the clock, not solved the problem.
I want to be careful and honest about the evidence here. The guideline endorsement of root-cause correction is a consensus position, not a stack of relapse-prevention trials. It is rated high because the major bodies agree on it and because it is mechanistically sound, not because someone ran a big randomized trial proving it. That is the most intellectually honest way I can put it.
What this means for the woman in front of me: before you buy a single repair supplement, the highest-value question is what slowed your gut or changed your terrain. That conversation belongs with your own provider, because the answer is specific to you, and it is the part most likely to change whether this comes back.
Is motility really the most important part of gut repair?
Motility is the part most worth your attention. The migrating motor complex is the wave that sweeps the small intestine clean between meals, like a housekeeping crew that only runs when you stop eating. When it stalls, bacteria are not cleared, and they regrow. Most serious relapse-prevention thinking centers on motility for exactly this reason (Deloose 2012).
Cross-section of the small intestine showing the migrating motor complex sweeping bacteria downstream between meals
Cross-section of the small intestine showing the migrating motor complex sweeping bacteria downstream between meals
Let me translate the mechanism, because this is the lever. Phase three of the migrating motor complex is the strong cleansing wave that runs in the fasting state, meaning when you are not eating and not snacking. It physically moves residue and bacteria from the small bowel toward the colon. Constant grazing, certain medications, and slowed nerve signaling can blunt it. When the housekeeping wave does not run, the small bowel becomes a place where bacteria can settle and multiply.
Now here is where I have to be straight with you, because this is where competitor protocols overreach. The mechanism is strong. The medications used to support motility, the prokinetics, have not been tested in formal relapse-prevention trials. There is no outcome study I have come across showing a specific prokinetic prevents SIBO from coming back. The biology is compelling and the clinical reasoning is sound. The proof for any particular agent preventing relapse is simply not there yet, and anyone who tells you otherwise is stating clinical experience with the confidence of a trial.
Two things I will add that the drug conversation skips, because this is the lever and you deserve the natural options too. First, the natural prokinetic. Ginger speeds up stomach emptying in human trials (Hu 2011), which is why it sits in so many motility protocols, including the one I trained on. The same honesty applies as for the drugs: that is gastric-emptying evidence, the small-bowel housekeeping-wave effect is extrapolated, and no trial shows ginger prevents relapse. A herbal blend called Iberogast is also used for sluggish digestion, though a trial found its benefit does not come from speeding emptying, so I hold it as traditional support, not a motility fix.
Second, and this is the free one nobody sells you. The housekeeping wave only runs when you are not eating. So leaving four to five hours between meals and a twelve-hour overnight fast, instead of grazing all day, is the simplest way to actually let it run. It costs nothing, it has the mechanism on its side, and it is the first thing on the protocol I trained with, ahead of any supplement.
Bolded micro-summary: motility is the mechanistically central lever for preventing regrowth, and finding your root cause is the guideline-backed durable fix. Those two together are the spine. Everything else is support with weaker evidence.
Should I take probiotics to rebuild my gut after antibiotics?
Reaching for a probiotic to reseed your gut after antibiotics is not the obvious fix it sounds like, and the best human study on this raises a real flag. An 11-strain probiotic delayed gut microbiome recovery for months after antibiotics, versus faster spontaneous rebound (Suez 2018, Cell). That finding surprises almost everyone, because it runs against the model most people absorbed.
Let me walk through that study plainly, because the headline matters less than what they actually did. Researchers gave people antibiotics, then split them into groups. One group took a multi-strain probiotic. Another recovered on their own. A third received an autologous fecal transplant, meaning a transfer of the person’s own gut bacteria, banked before the antibiotics. The probiotic group’s own native gut bacteria took longer to come back, for months, than the group that simply recovered on its own. The intuitive “antibiotics deplete, probiotics replace” picture did not hold.
I do not want to overstate this, so here is the honest calibration. The field is not settled. That study enrolled twenty-one people, used invasive sampling, and measured the lining microbiome rather than how anyone felt. It is one rigorous signal, not the final word. And probiotics do have one narrow, well-supported job: specific high-dose strains reduce antibiotic-associated diarrhea (Cochrane, Guo 2019). That is real and worth knowing. It is just not the same as rebuilding your microbiome. The claim is not “probiotics are bad.” The claim is that the reflexive reseed is oversold, and the one thing it reliably does is narrower than the marketing implies.
What this means for the woman in front of me: if you have been told to load probiotics to “put the good bacteria back,” it is reasonable to pause and ask which job you are actually buying. Reducing antibiotic diarrhea is a real use. Rebuilding your terrain is not a promise the strongest study supports.
I went deep on why strain and dose decide whether a probiotic does anything at all in why your probiotic isn’t working, and which one might. The short version is that “take a probiotic” is not a strategy. The specifics are the whole thing.
Can glutamine heal my gut lining?
Glutamine is the most-studied lining-support nutrient, and the honest evidence is mixed with one genuinely promising trial. Glutamine 5 g three times daily beat placebo 80% to 6% on symptoms in post-infectious IBS (Zhou 2018). That is a striking result. It also was not done in a post-SIBO-treatment population, and that distinction is the whole point.
First, the mechanism, because the lining question deserves a clear picture. Your gut lining is real and it does repair itself. The cells that line the intestine regenerate from stem cells tucked in the crypts, the small folds of the gut wall. The junctions between those cells then reseal. Think of the barrier like a tight glass mosaic: the pieces are held in a frame, and the seals between them control what passes through. When the seals loosen, the picture is what people mean by “leaky gut.” Glutamine is fuel and raw material the lining cells use. In the lab it raises the proteins that tighten those seals.
Now the honest part. When you pool the human trials across adults, glutamine shows no clear overall effect on the barrier (Abbasi 2024). The one clean positive result came in people with post-infectious IBS who had a documented leaky barrier, not in people finishing SIBO treatment. So the fair statement is this. Glutamine is the most-studied option, it is mechanistically reasonable, and it has one good trial in a neighboring condition. It is not proven for your exact situation. I would rather tell you that than sell you certainty I do not have.
A note on the “leaky gut” label, because it gets abused. Intestinal permeability is a real mechanism. “Leaky gut syndrome” is not a formal diagnosis with a validated test, and the label is overused to sell things. The mechanism is worth understanding. The marketing built on top of it usually is not.
If you are still sorting out what your breath test actually told you before you build any repair plan, I broke down the testing in methane SIBO and breath-test literacy.
Bolded micro-summary: the lining genuinely repairs itself from crypt stem cells. Glutamine supports that biology and has one strong adjacent-population trial, but the overall human evidence is null and it is unproven for the post-SIBO setting.
What about marshmallow root, slippery elm, and DGL for the gut lining?
Demulcent herbs like marshmallow root, slippery elm, and DGL have a long traditional history of soothing an irritated gut lining. They are traditionally used, not trial-proven for repair, and I think that honest distinction is exactly what is missing from most rebuild content. A demulcent, meaning a plant that forms a soothing, slippery coating, is a category herbalists have leaned on for generations.
DGL is deglycyrrhizinated licorice, meaning licorice with the compound that raises blood pressure removed. That removal matters, and I will come back to it in the safety section. Marshmallow root and slippery elm are mucilage herbs, plants rich in a gel-like fiber that coats irritated tissue. The traditional rationale is real and old. The controlled human gut-repair trials are essentially absent. I am not going to pretend a tradition is a trial.
I hold these plants with respect. Marshmallow root is a beautiful, genuinely soothing herb, and tradition is a legitimate form of knowledge that I name out loud rather than bury. But naming it honestly means saying the evidence tier is traditional, not proven, so you can decide with clear eyes instead of marketing gloss.
What this means for the woman in front of me: demulcents are reasonable, low-drama, traditionally used comfort support, not a proven repair fix. If they help you feel better while the real work happens on motility and root cause, that is a fair use, named for what it is.
Does perimenopause make SIBO harder to rebuild from?
For women in their late thirties and into their forties, there is a thread worth naming gently. The decline in estrogen and progesterone may slow the migrating motor complex, the same housekeeping wave covered earlier, and that could feed recurrence. This is mechanistically plausible and I want to be careful not to oversell it, because no trial has nailed it down.
Here is the honest framing. Sex hormones influence gut motility, and motility is the lever that keeps the small bowel swept clean. As those hormones shift in perimenopause, meaning the years of hormonal change before periods stop, it is reasonable to wonder whether a slower wave makes relapse more likely. That is a hypothesis with mechanism behind it, not a proven cause. I have seen the perimenopause-gut overlap come up often in cases I’ve reviewed, and the research thread is young.
I wrote about the hormone-gut connection in more depth in the estrogen-gut-vascular axis in perimenopause. If you are rebuilding while your hormones are also shifting, that piece is the bridge.
Bolded micro-summary: the perimenopause-motility-recurrence link is plausible and worth raising with your provider, but it rests on mechanism, not a randomized trial. Treat it as a question to explore, not a settled cause.
What I’d do this week
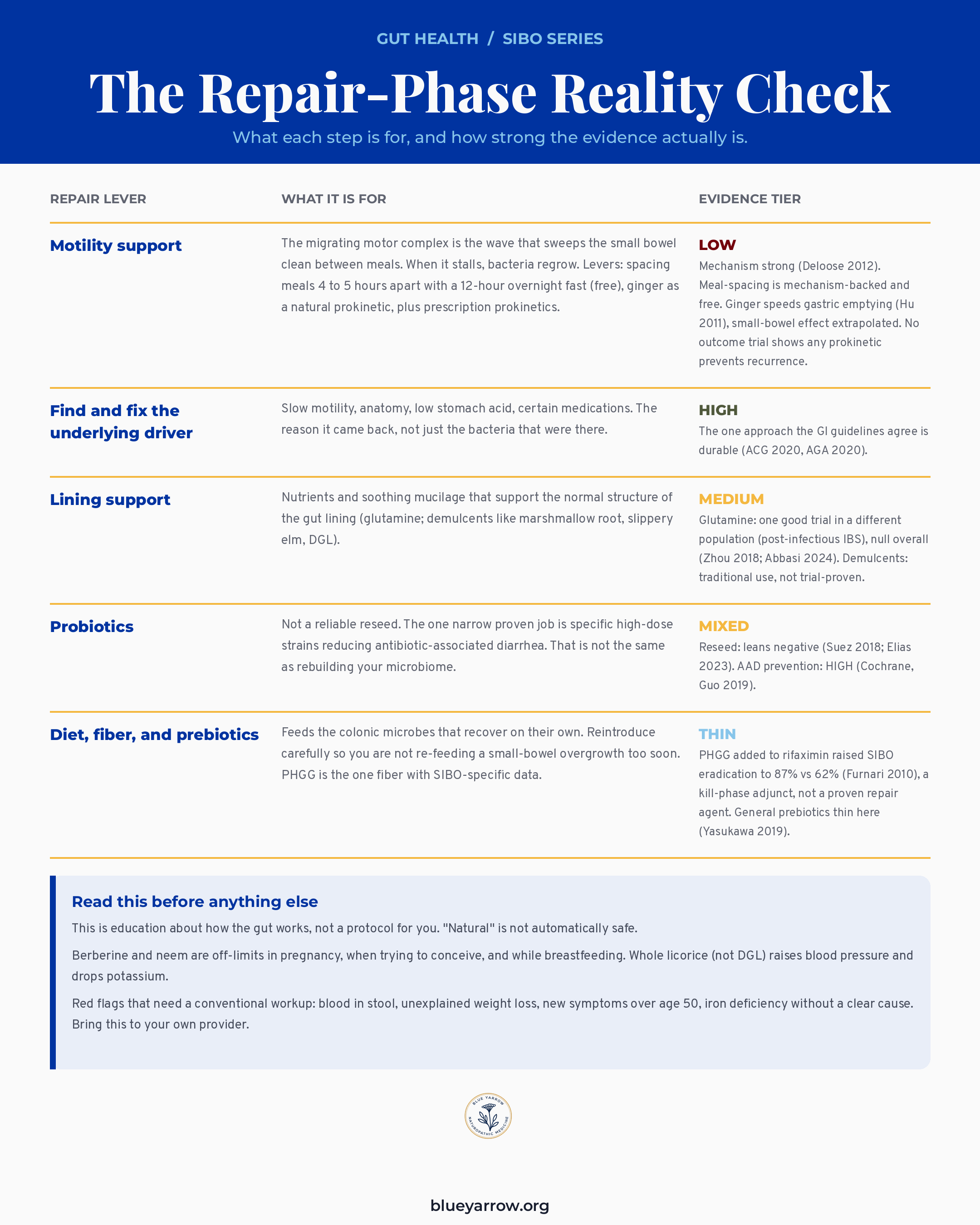
I cannot give you a protocol, because a protocol for a specific person is a clinical decision that belongs with your own provider. What I can give you is the map I wish someone had handed you after the kill phase: what each repair lever is actually for, and how strong the evidence behind it really is. Save this. It is the part that does not change with the next supplement trend.
Repair-Phase Reality Check chart listing five gut-repair levers with their plain mechanism and honest evidence tier
Repair-Phase Reality Check chart listing five gut-repair levers with their plain mechanism and honest evidence tier
The honest bottom line on rebuilding your gut
So here is what I want you to walk away with, empowered to ask sharper questions and a little harder to sell to. The kill phase cleared the overgrowth, and you did everything right. It comes back for close to half of people, and the rebuild you were sold is mostly mechanism and marketing, not proof. The durable work is restoring motility and finding the root cause of why the bacteria overgrew, and being honest about which repair steps have evidence behind them and which are tradition or hope.
That is a less satisfying answer than a numbered supplement stack. I think it is also the true one. And the true one respects what you have already spent: money, effort, and the quiet grief of doing everything right and watching it return. You were not failing the protocol. You were handed half of one.
If you finished antibiotics or herbal antimicrobials and it came back, what is the one thing no provider has actually explained to you about why? Tell me, and I will keep writing the pieces that fill that gap.
Frequently asked questions
How long does it take to rebuild your gut after antibiotics? The microbiome usually begins rebounding within about a week, but the return is often incomplete and individual, settling over weeks to months. There is no fixed timeline. The honest answer is that recovery is partial and personal, and the bigger driver of lasting results is correcting why the overgrowth happened, not the calendar.
Should I take probiotics during or after antibiotics for SIBO? For rebuilding your microbiome, the strongest human study found a multi-strain probiotic actually delayed recovery of your own gut bacteria (Suez 2018). Probiotics do have one narrow, proven job: specific high-dose strains reduce antibiotic-associated diarrhea (Cochrane, Guo 2019). That is a real use, but it is not the same as reseeding your gut.
Does glutamine actually heal leaky gut? Glutamine supports the lining biologically and helped in one good trial of post-infectious IBS at 5 grams three times daily (Zhou 2018). When you pool the human trials across adults, the overall effect on permeability is null (Abbasi 2024). So it is the most-studied option and mechanistically reasonable, but unproven for the post-SIBO setting specifically.
Why does my SIBO keep coming back even when I’m strict? Recurrence is common because antibiotics clear the bacteria without changing why they overgrew. Close to half of patients relapse within nine months of one antibiotic course (Lauritano 2008). Strictness with diet does not fix slowed motility, anatomy, low stomach acid, or a contributing medication, which are the underlying drivers guidelines point to.
Does ginger or a natural prokinetic help with the motility part? Ginger speeds up stomach emptying in human trials (Hu 2011), which is why it appears in many motility protocols. Be clear on the tier, though: that is gastric-emptying evidence, the small-bowel housekeeping-wave effect is extrapolated, and no trial shows ginger prevents SIBO from coming back. The free, mechanism-backed move is spacing your meals four to five hours apart with a twelve-hour overnight fast, because the cleaning wave only runs when you are not eating.
Is “leaky gut” a real diagnosis? Intestinal permeability is a real, measurable mechanism. “Leaky gut syndrome,” as a standalone diagnosis with a validated test, is not formally recognized, and the label is widely overused to sell supplements. The mechanism is worth understanding. Most of the marketing built on the phrase outruns the actual evidence.
Is it safe to keep taking antimicrobial herbs while trying to conceive? No. Berberine and neem are contraindicated in pregnancy, when trying to conceive, and while breastfeeding, and whole licorice raises blood pressure and drops potassium. “Natural” does not mean automatically safe, and the reproductive-safety data on many of these herbs is thin. Bring any plan to your own provider before continuing.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Lauritano, E. C., et al. (2008). Small intestinal bacterial overgrowth recurrence after antibiotic therapy. American Journal of Gastroenterology, 103(8), 2031-2035. PMID: 18802998
2. Suez, J., Zmora, N., Zilberman-Schapira, G., et al. (2018). Post-antibiotic gut mucosal microbiome reconstitution is impaired by probiotics and improved by autologous FMT. Cell, 174(6), 1406-1423. PMID: 30193113. https://doi.org/10.1016/j.cell.2018.08.047
3. Zhou, Q., Verne, M. L., Zhang, B., & Verne, G. N. (2018). Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome. Gut, 68(6), 996-1002. PMID: 30108163
4. Abbasi, F., Haghighat Lari, M. M., Khosravi, G. R., et al. (2024). A systematic review and meta-analysis of clinical trials on the effects of glutamine supplementation on gut permeability in adults. Amino Acids, 56, 60. PMID: 39397201
5. Éliás, A. J., Barna, V., Patoni, C., et al. (2023). Probiotic supplementation during antibiotic treatment is unjustified in maintaining the gut microbiome diversity: a systematic review and meta-analysis. BMC Medicine, 21, 262. PMID: 37468916
6. Guo, Q., Goldenberg, J. Z., Humphrey, C., El Dib, R., & Johnston, B. C. (2019). Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database of Systematic Reviews, (4), CD004827. PMID: 31039287. https://doi.org/10.1002/14651858.CD004827.pub5
7. Deloose, E., Janssen, P., Depoortere, I., & Tack, J. (2012). The migrating motor complex: control mechanisms and its role in health and disease. Nature Reviews Gastroenterology & Hepatology, 9(5), 271-285. https://doi.org/10.1038/nrgastro.2012.57
8. Pimentel, M., et al. (2020). ACG Clinical Guideline: small intestinal bacterial overgrowth. American Journal of Gastroenterology, 115(2), 165-178. PMID: 32023228
9. Quigley, E. M. M., Murray, J. A., & Pimentel, M. (2020). AGA Clinical Practice Update on small intestinal bacterial overgrowth. Gastroenterology, 159(4), 1526-1532. https://doi.org/10.1053/j.gastro.2020.06.090
10. Yasukawa, Z., Inoue, R., Ozeki, M., et al. (2019). Effect of repeated consumption of partially hydrolyzed guar gum on fecal characteristics and gut microbiota. Nutrients, 11(9), 2170. PMID: 31509971
11. Hu, M. L., Rayner, C. K., Wu, K. L., et al. (2011). Effect of ginger on gastric motility and symptoms of functional dyspepsia. World Journal of Gastroenterology, 17(1), 105-110. https://doi.org/10.3748/wjg.v17.i1.105
12. Furnari, M., Parodi, A., Gemignani, L., et al. (2010). Clinical trial: the combination of rifaximin with partially hydrolysed guar gum is more effective than rifaximin alone in eradicating small intestinal bacterial overgrowth. Alimentary Pharmacology & Therapeutics, 32(8), 1000-1006. https://doi.org/10.1111/j.1365-2036.2010.04436.x
13. Braden, B., Caspary, W., Borner, N., Vinson, B., & Schneider, A. R. J. (2009). Clinical effects of STW 5 (Iberogast) are not based on acceleration of gastric emptying in patients with functional dyspepsia and gastroparesis. Neurogastroenterology & Motility, 21(6), 632-638. https://doi.org/10.1111/j.1365-2982.2008.01249.x
14. SUHS / Sonoran University naturopathic clinical training, SIBO treatment protocol (Dr. Shad Abdulla, ND). [Naturopathic clinical training: meal-spacing and overnight-fast motility practice, ginger prokinetic, PHGG/Sunfiber, herbal antimicrobials, lining support.]