Why Your Methane Breath Test Isn’t the Same as SIBO
If you just got your breath test back and you are staring at a chart of numbers nobody explained, let me read it with you. One clinician calls it SIBO. Another waves it off as “just IBS-C.” Here is the calm version first. A methane result is its own thing, with its own organism and its own meaning, and you can learn to read it without spiraling.
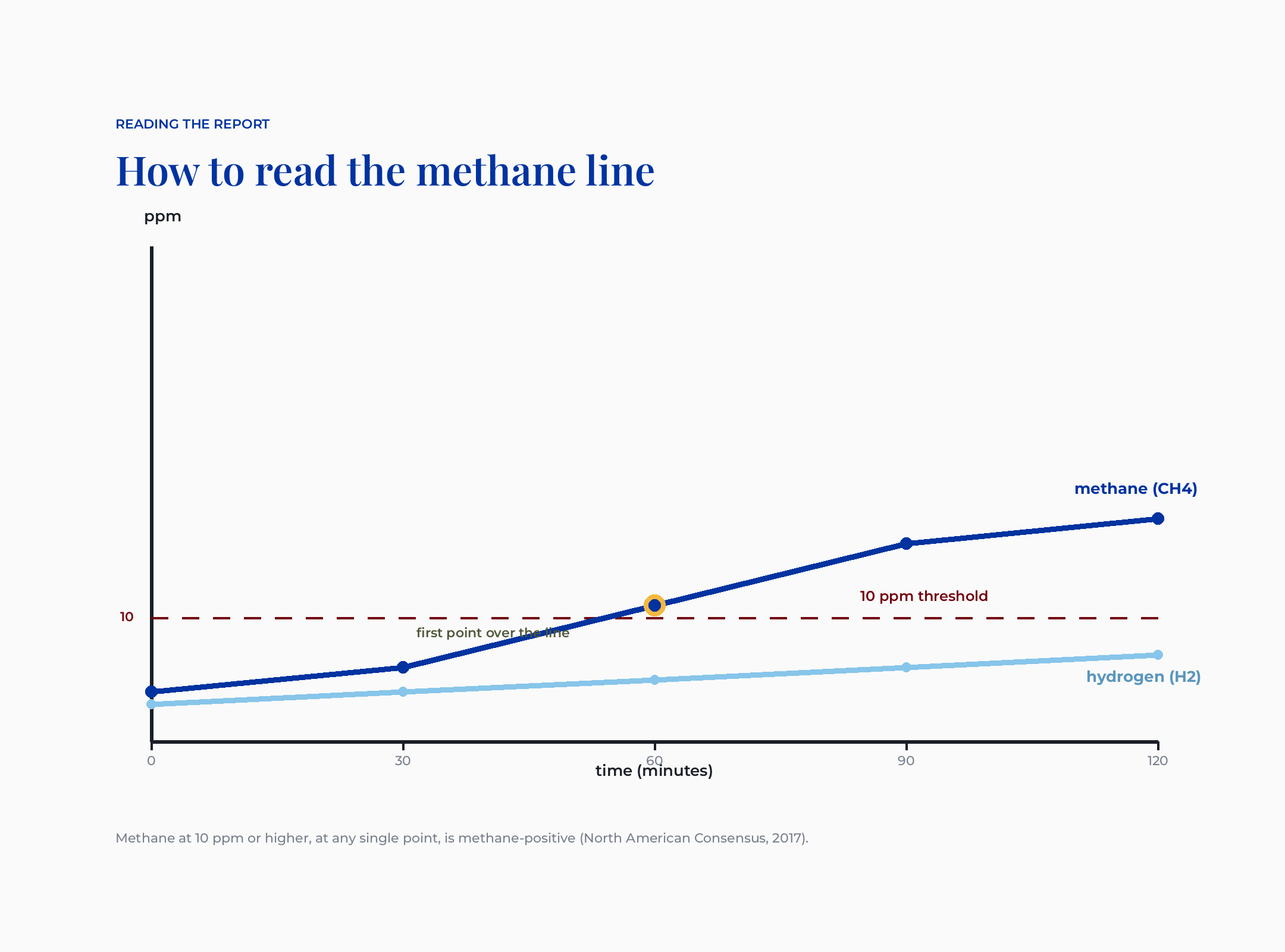
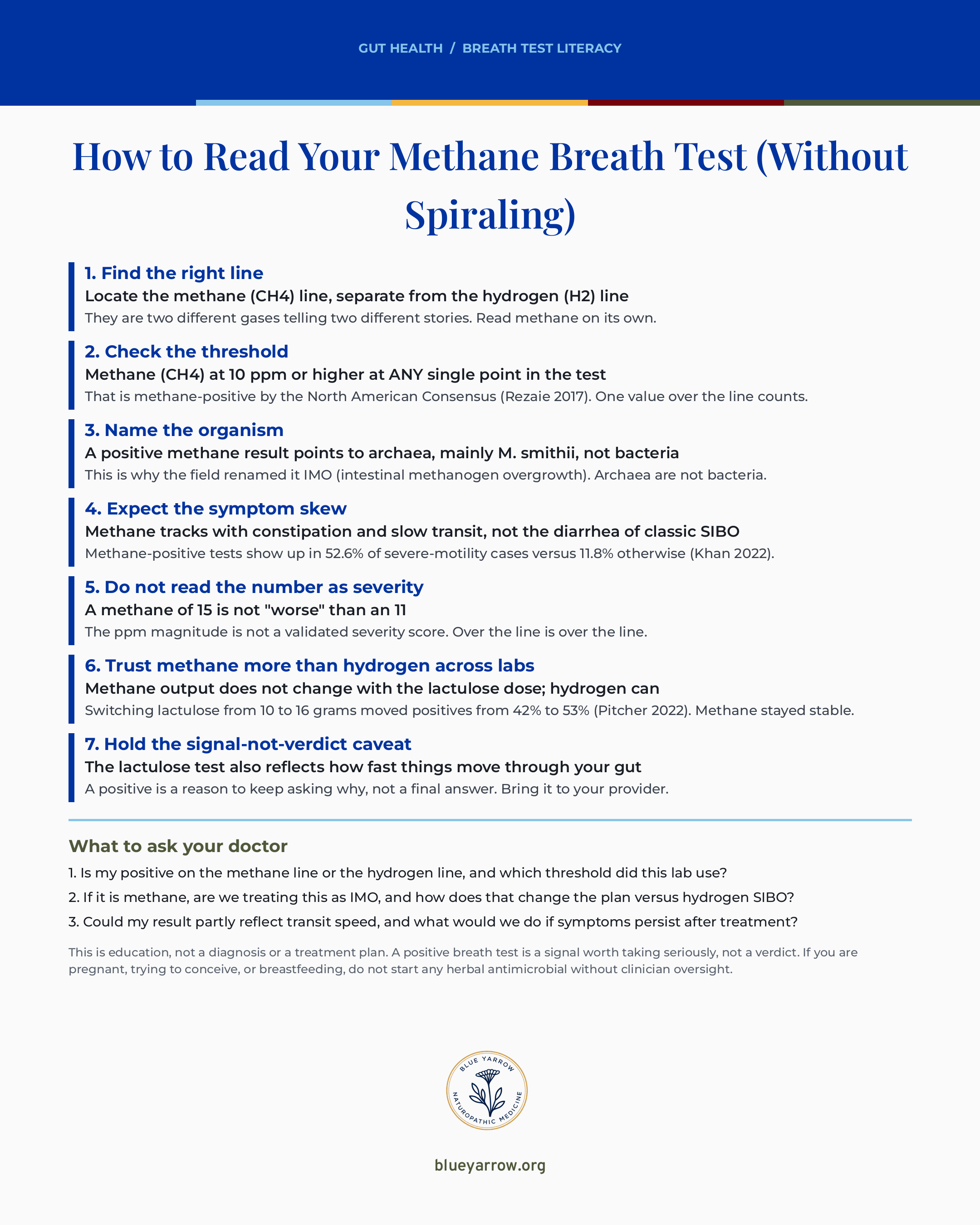
Methane at 10 ppm or higher, at any point, is a positive result (North American Consensus, 2017). That single line is the answer to the question you typed into the search bar. Everything else on the page builds out from there.
I am Dr. Shad Abdulla, ND, a naturopathic doctor who reads the actual trials instead of the supplement label. In cases I’ve reviewed, the breath-test report is the document that scares women most, because no one sits down and translates it. So that is what I am going to do here.
This walks through how to find the right line on your report and what the 10 ppm threshold means. It covers why the number is not a severity score, and gives you one save card for your next appointment. Let me back up and explain what this chart is really showing you.
What does a methane breath test actually measure?
A methane breath test measures one gas in your breath over a few hours after you drink a sugar called lactulose. Lactulose is a sugar your own body cannot absorb. So it travels down to the microbes in your gut, who ferment it and release gases you then breathe out. The test counts those gases in parts per million, or ppm, meaning how many gas molecules show up per million molecules of breath.
Here is the part conventional medicine often skips. The report has two separate lines, hydrogen and methane, and they tell two different stories. Most women are handed the whole curve as if it were one verdict. It is not.
What this means for the woman in front of me is simple. Before you panic about a “positive,” you need to know which line went positive and what that specific line points to. The root-cause version of this question is not “do I have SIBO,” it is “which gas, which organism, and why is my gut making it.”
Where is the methane line on my report, and what counts as positive?
Find the line labeled methane, or CH4, and read it on its own, separate from the hydrogen line. Methane at 10 ppm or higher, at any point, is a positive result (North American Consensus, 2017). One value over the line counts. It does not have to climb or hold; a single point at or above 10 ppm is enough.
That 10 ppm cutoff comes from a 2017 consensus of seventeen gastroenterology researchers who agreed on how to read these tests. It is the closest thing this field has to a rulebook. So when your lab flags methane, this is the threshold it is using.
A quick note on the hydrogen line, because it confuses people. Hydrogen is read differently. A rise of 20 ppm or more by ninety minutes is the SIBO-positive marker on that line. The two gases do not share a cutoff, and they do not mean the same thing.
What this means for you is that “my methane was high but my hydrogen was normal” is a real and common pattern, not a mistake. It is pointing you toward a specific entity, which is the next thing to understand.
Why is methane SIBO now called IMO?
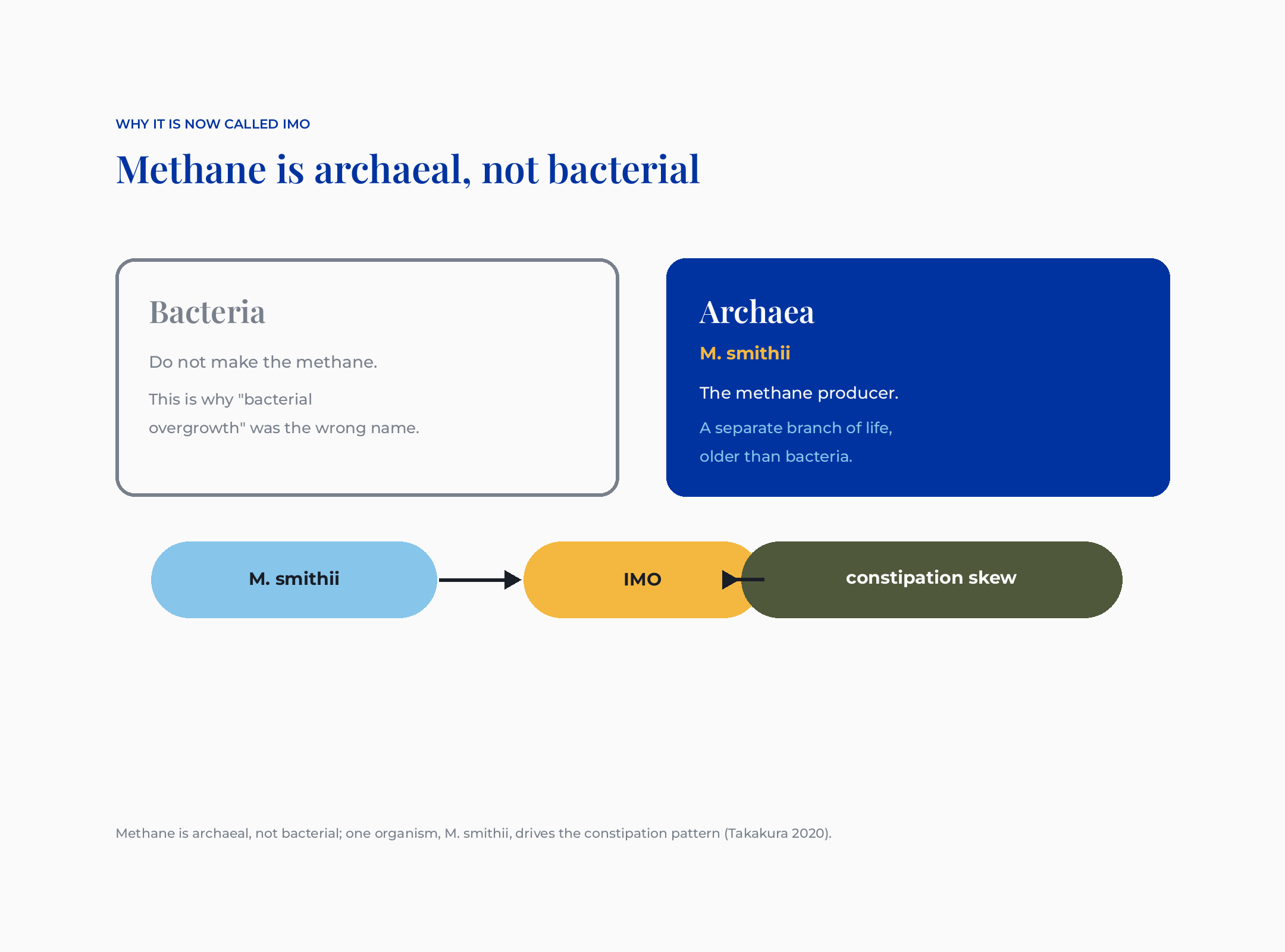
Because methane is not made by bacteria. Methane is archaeal, not bacterial; one organism, M. smithii, drives the constipation pattern (Takakura 2020). Archaea are a separate branch of microbial life, older than bacteria and biologically distinct, and Methanobrevibacter smithii, usually shortened to M. smithii, is the main methane producer in the human gut.
That is why the field renamed this condition. IMO stands for intestinal methanogen overgrowth, meaning an overgrowth of these methane-making archaea. The old label “methane SIBO” had bacteria right in the name, which was misleading. The thing driving your number is not a bacterium at all.
I want you to understand why this rename matters for you, not just for a textbook. Maybe a clinician told you your label changed. Maybe you saw “IMO” on a newer report and panicked that it was something new and worse. It is not. It is the same finding, named more accurately. The naturopathic lens on this is that naming the actual organism changes how I think about the next steps. Archaea and bacteria do not behave the same way.
Here is a vignette, and her name and details are changed for confidentiality, of course. A woman I’ll call Priya wrote to me holding two reports a year apart. One said “methane-positive SIBO,” the newer one said “IMO,” and she was convinced she had developed a second disease. She had not. Same archaea, same gut, updated vocabulary. The relief on that one was immediate.
Does a positive methane test mean constipation or diarrhea?
Methane tracks with constipation and slow transit, not the diarrhea that people associate with classic SIBO. This is one of the most useful things to know when you read your own report, because it reframes the whole picture. If you have been bloated and constipated and someone kept treating you for a diarrhea-type overgrowth, the gas pattern may explain the mismatch.
The reason is mechanical. Methane appears to act directly on the smooth muscle of the gut to slow things down. That is why methane-positive results show up so heavily in people with severe slow-transit problems. In one study of a serious motility disorder, methane-positive tests appeared in 52.6% of cases versus 11.8% of people without it.
I will be honest about the limit here, because it matters. That methane slows transit is well supported as a mechanism. That clearing methane will reliably fix any given person’s constipation is plausible but not settled in trials. The association is real and directional; the cause-and-effect loop is not nailed down.
What this means for the woman in front of me is that the constipation and the methane are linked. That link is worth taking seriously. But it is not a promise that one number controls your symptoms. Hold both.
This is also where the dismissal wounds people. If you have been told it is “just IBS-C, take magnesium,” that is not wrong exactly, but it is incomplete. IMO is a defined entity with a specific organism and a measurable signal. You are allowed to want a fuller answer than magnesium and a shrug. For more on how the constipation-predominant labels themselves got redrawn, I walk through the Rome V reclassification of IBS in a separate piece.
Is a higher methane number a worse case?
No. A methane of 15 is not “worse” than a methane of 11. The ppm magnitude is not a validated severity score. Over the line is over the line. This is the single most common misread I see, and it generates a lot of unnecessary fear.
It is an understandable mistake. Bigger number, worse problem, that is how most lab values work. But methane positivity is a yes-or-no signal at the 10 ppm threshold, not a dial that measures how sick you are. No study grades severity by the size of the number.
Here is a second vignette, details changed for confidentiality. A woman I’ll call Dana came to a question thread terrified. Her methane peaked at 38, and a forum had told her that meant “severe.” It did not. A 38 and an 11 cross the same line into the same category. Her anxiety was real; the severity reading was not.
What I want you to do with this is stop ranking yourself by the height of the curve. The number told you that you are methane-positive. It did not tell you that you are a worse case than the woman next to you.
Why do different labs give me different results?
Because the labs do not all run the same test the same way, especially on the hydrogen side. Switching lactulose from 10 to 16 grams raised positive results from 42% to 53% (Pitcher 2022). That means the same person could read positive at one lab and negative at another, purely because of how much sugar the lab used.
Here is the reassuring part, and it is the root-cause version of “which number do I trust.” Methane is the steadier line. Methane production does not change with the lactulose dose the way hydrogen does. So your methane reading holds up across labs far better than your hydrogen reading. In cases I’ve reviewed, the methane line is the one I lean on when two reports disagree.
So if you compare a hydrogen result from two labs and they do not match, that is not necessarily an error in either. It is the protocol. The methane line gives you firmer ground to stand on.
What this means for you is concrete. When you bring your report to your provider, you can ask which substrate dose the lab used. And when the two lines conflict, you can put more weight on the methane finding than the hydrogen one.
Does a positive test mean I definitely have an overgrowth?
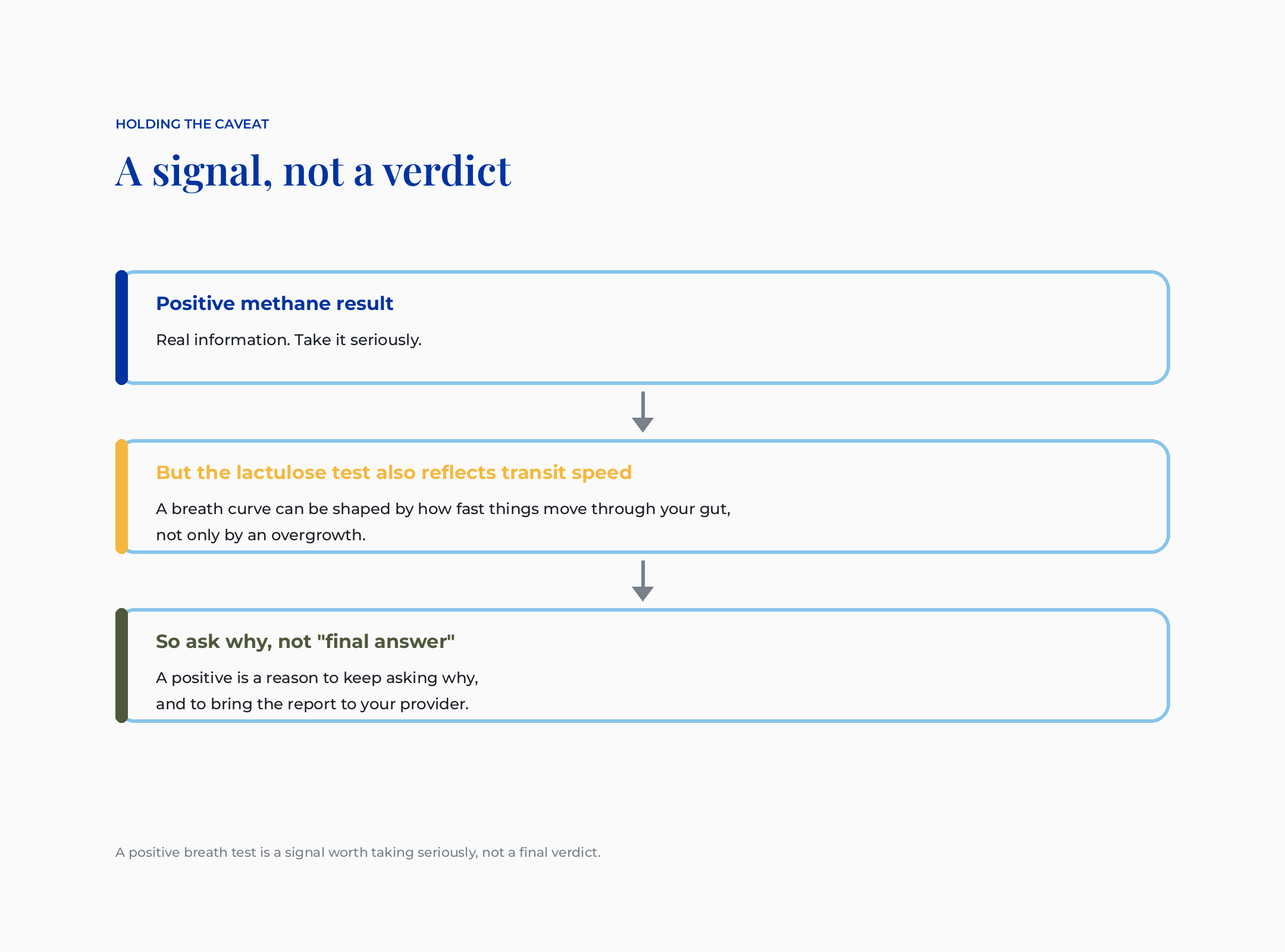
Not by itself. A positive breath test is a signal worth taking seriously, not a final verdict. Conventional medicine misses something when it treats the test as settled. So does the functional-medicine world when it treats the result as a clean diagnosis you can clear with the perfect protocol.
The lactulose test also reflects how fast things move through your gut. A breath curve can be shaped by your transit speed, not only by an overgrowth. That is why a positive is a reason to keep asking why, rather than a closed case. The honest reading sits between the two camps. The test is useful, and it is contested.
I hold this tension on purpose, because it is the truth, and because naming uncertainty is more trustworthy than pretending the instrument is perfect. The same research group authored much of both the criteria and the validation for these tests. That is worth knowing, not to dismiss the work, but to stay humble about it.
What this means for the woman in front of me is the calmest and most freeing frame of all. Your positive is real information. It is not a life sentence and it is not a complete explanation. It is the start of a better conversation, not the end of one. For the bigger picture on why these overgrowths return, I go deeper in SIBO subtypes and why it keeps coming back.
What about treatment, and where do herbs fit?
Treatment is a secondary note here, because this piece is about reading your report, not starting a protocol. But I will be honest about what the evidence shows so you are not left guessing. For methane-positive cases, the most studied antibiotic approach pairs rifaximin with neomycin rather than rifaximin alone. Rifaximin is a gut-targeted antibiotic; neomycin is a second antibiotic that the data suggests adds methane coverage.
I say “most studied,” not “best,” and the distinction is deliberate. The combination evidence is retrospective, not a randomized trial, so it is the most examined approach rather than a proven winner. No single antimicrobial dominates for methane.
On the botanical side, this is where my herbalist training and my caution sit together. The literature studies berberine-containing plants, oregano oil, and allicin from garlic for methanogen suppression, and there is real traditional digestive use behind the berberine plants. But the trials matching the antibiotic eradication data are limited or absent, so I name that honestly rather than overselling the herbs.
One hard safety line, because my audience is women of reproductive age. If you are pregnant, trying to conceive, or breastfeeding, do not start berberine, oregano oil, or any herbal antimicrobial without clinician oversight. Berberine in particular carries real drug interactions and a bilirubin concern that make the “natural so it is safe” assumption wrong here. This is education about what the literature studies, not a protocol to start alone. Maybe a botanical or a probiotic that worked for a friend does nothing for you. The strain and the target matter, which I cover in why your probiotic isn’t working and which one might.
What I’d do this week
If you are holding a confusing report right now, here is the one bookmarkable thing to take with you. Read your methane line using this card, then bring the three questions to your provider. Save this for your next appointment.
The calm version of all this
If you have come this far, thank you. Here is what I want you to walk away holding. Your methane line is its own story, with its own threshold, its own organism, and its own symptom skew. A positive number is real and worth taking seriously, and it is a signal rather than a verdict. You can read your own report now, a little harder to fool, and a lot less alone with it.
What did your doctor tell you when you asked about your breath test, and did it match what you see on the page now?
Frequently asked questions
Is methane SIBO the same as IBS-C? They overlap, but they are not the same thing. IBS-C is a symptom-based label for constipation-predominant irritable bowel. IMO, the methane overgrowth, is a specific finding with a measurable gas and a known organism. Calling a methane-positive result “just IBS-C” is an oversimplification, not a full answer.
What methane level is considered positive on a breath test? Methane at 10 ppm or higher, at any single point during the test, is methane-positive by the North American Consensus. The value does not need to rise or hold. One reading at or above 10 ppm meets the threshold, while the hydrogen line uses a separate rule entirely.
Is a higher methane number more dangerous? No. The ppm number is a yes-or-no threshold marker at 10 ppm, not a severity score. A methane of 30 is in the same category as a methane of 11. No study grades how sick you are by the size of the number, so try not to rank yourself by the height of the curve.
Why is methane SIBO now called IMO? Because methane is made by archaea, not bacteria, so “bacterial overgrowth” was the wrong name. IMO stands for intestinal methanogen overgrowth and names the actual organism, Methanobrevibacter smithii. The finding did not change. The vocabulary got more accurate.
Can I trust a positive breath test completely? Take it seriously, but not as a closed case. The lactulose test partly reflects how fast things move through your gut, so transit speed can shape the curve. Your positive is real information and a reason to keep asking why, which is why the next step is a conversation with your provider.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Rezaie, A., Buresi, M., Lembo, A., Lin, H., McCallum, R., Rao, S., … Pimentel, M. (2017). Hydrogen and methane-based breath testing in gastrointestinal disorders: The North American Consensus. The American Journal of Gastroenterology, 112(5), 775 to 784. https://doi.org/10.1038/ajg.2017.46
2. Takakura, W., & Pimentel, M. (2020). Small intestinal bacterial overgrowth and irritable bowel syndrome: An update. Frontiers in Psychiatry, 11, 664. https://doi.org/10.3389/fpsyt.2020.00664
3. Barlow, G. M., & Pimentel, M. (2025). Modern concepts of small intestinal bacterial overgrowth. Current Opinion in Gastroenterology, 41(6), 399 to 408. https://doi.org/10.1097/MOG.0000000000001135
4. Khan, M. Z., Lyu, R., McMichael, J., & Gabbard, S. (2022). Chronic intestinal pseudo-obstruction is associated with intestinal methanogen overgrowth. Digestive Diseases and Sciences, 67(10), 4834 to 4840. https://doi.org/10.1007/s10620-021-07343-1
5. Pitcher, C. K., Farmer, A. D., Haworth, J. J., Treadway, S., & Hobson, A. R. (2022). Performance and interpretation of hydrogen and methane breath testing impact of North American Consensus guidelines. Digestive Diseases and Sciences, 67(12), 5571 to 5579. https://doi.org/10.1007/s10620-022-07487-8
6. Low, K., Hwang, L., Hua, J., Zhu, A., Morales, W., & Pimentel, M. (2010). A combination of rifaximin and neomycin is most effective in treating irritable bowel syndrome patients with methane on lactulose breath test. Journal of Clinical Gastroenterology, 44(8), 547 to 550. https://doi.org/10.1097/MCG.0b013e3181c64c90