Will a Probiotic Cure Your Yeast Infection?
If you have been told it is normal to get a yeast infection now and then, and you are now on your fifth, your eighth, your tenth, I want to start somewhere most content for this problem refuses to start. With the honest answer.
A probiotic will not clear an active yeast infection on its own. The antifungal does that work. What the research supports is a smaller role: added to an antifungal, probiotics may modestly help short-term and lower one-month recurrence, but that benefit fades and the whole evidence base is weak. I am Dr. Shad Abdulla, ND, and I read these trials in full so I can tell you the size of the effect, not just sell you on the idea of it.
Here is what conventional medicine gets right and still leaves you with. It says the antifungal is the cure and probiotics are not proven, then sends you home, and the infection comes back. Here is what the wellness aisle gets wrong. It sells the opposite story, that a daily probiotic and an anti-sugar cleanse will fix the root cause, and it oversells a tool the trials do not back. The honest position sits between them. In this piece I will walk you through what the evidence actually shows, when a probiotic is worth it, when it is not, and the question almost nobody asks first: is it even yeast?
Bottom line up top: probiotics are a weak adjunct, useless against an active infection, and often the wrong tool for what is actually something else.
What conventional care misses (and what the wellness aisle gets wrong)
Conventional care misses the part that matters most to you, which is recurrence. The antifungal clears the episode in front of you, and the data on that are strong. Azoles, meaning the fluconazole pill or the topical creams in that class, cure roughly 80 to 90 percent of uncomplicated infections, and every major guideline puts them first (CDC, ACOG, IDSA, NICE, AAFP). But once you are on your tenth round, the episode is not the disease. The pattern is. And the standard visit rarely sits with you long enough to ask why the pattern keeps repeating.
That gap is exactly where the wellness aisle moves in. It hands you a daily probiotic, a “starve the yeast” diet, and the promise of a root-cause fix. The pull is understandable. You want the cause addressed, not just the symptom muted. The problem is that the product is sold far ahead of what the trials show, and that overpromise is its own kind of dismissal. It treats your hope as a marketing channel.
I want to give you the third thing, which is neither the brush-off nor the overpromise. Probiotics have a real but small place here, and naming that place honestly is more useful than either camp’s story. As a naturopathic doctor, my root-cause lens does not mean I reach for a supplement first. It means I ask what is actually driving the recurrence before anyone reaches for anything.
The honest read is the one neither side gives you: probiotics help a little, in a narrow window, and only as a sidekick to the drug.
What is a yeast infection, in plain terms
A yeast infection, what clinicians call vulvovaginal candidiasis, is an overgrowth of a yeast called Candida in the vaginal tissue, usually Candida albicans. Candida lives there normally in small amounts. The infection is what happens when it overgrows and your body reacts.
Here is the part that reframes everything. The burning, the itch, the rawness, those are not coming straight from the yeast count. They come from your own immune response. When Candida shifts into its thread-like hyphal form, it releases a toxin called candidalysin, which damages the surface cells and triggers an inflammatory reaction (Cheng 2024; Willems 2018). So the symptoms are immunopathology, meaning your immune system’s overreaction to the yeast, not simply the amount of yeast present.
Why does that matter to you? Because it explains why “kill more yeast” is not automatically the same as “feel better,” and why the tools that calm the tissue or restore the normal flora are part of a different conversation than the antifungal.
A yeast infection is a Candida overgrowth, but the misery you feel is largely your own inflammation responding to it.
What the evidence actually shows about probiotics
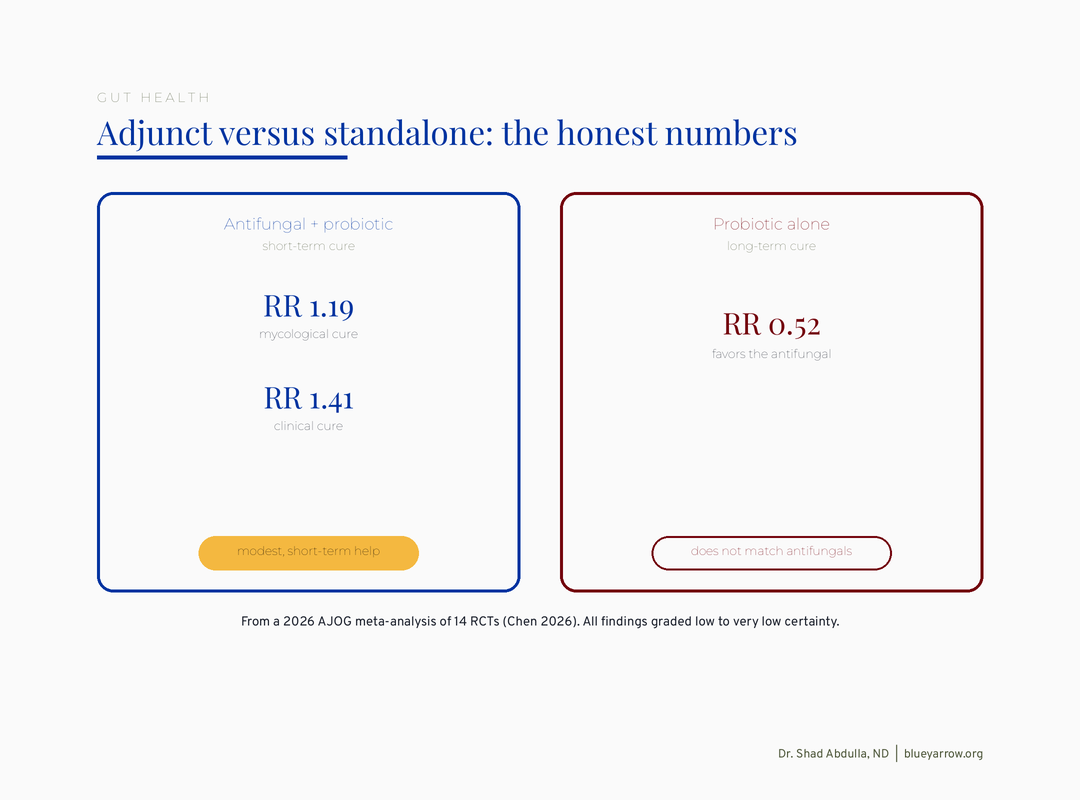
Here is the cleanest summary I can give you. Added to an antifungal, probiotics modestly improve short-term cure and cut one-month recurrence. On their own, they do not match antifungals for lasting cure. And the certainty behind all of it is low to very low. That is not me hedging. That is the grade the researchers themselves assigned.
Let me walk you through the studies the way I would if you were sitting across from me, because the numbers matter and the marketing never shows them.
The strongest review: the 2026 AJOG meta-analysis
In January 2026, a team published a meta-analysis in the American Journal of Obstetrics and Gynecology pulling together 14 randomized trials (Chen 2026). When a probiotic was added to an antifungal, short-term mycological cure, meaning the yeast actually cleared on lab testing, improved (RR 1.19). Clinical cure, meaning symptoms resolved, improved too (RR 1.41). But probiotics taken alone were inferior to antifungals for long-term cure (RR 0.52, favoring the drug). The authors graded every one of these findings low to very low certainty.
Probiotics alone lose to antifungals for lasting cure (RR 0.52 favoring the drug), per a 2026 AJOG meta-analysis.
The reference standard: the Cochrane review
Cochrane, the gold standard for this kind of synthesis, looked at 10 trials and over 1,600 women, all using probiotics as an add-on (Xie 2017). Short-term cure rates nudged up. One-month relapse dropped meaningfully (RR 0.34). But there was no lasting benefit, and again the certainty was low to very low.
Added to an antifungal, probiotics cut one-month yeast recurrence (RR 0.34), but the benefit fades (Cochrane 2017).
The gaps that should make you cautious
Now here is where it gets interesting, and where honesty matters most. The positive signals ride on very wide statistical ranges, the kind that show up when studies are small and the strongest results get published while the null ones go missing. When researchers restricted one 2026 analysis to only the most rigorous placebo-controlled trials, an apparent benefit collapsed to nothing (Liu 2026). And on the hardest endpoint, the actual culture result, a 2023 review found probiotics no different from placebo (Zahedifard 2023).
The trials also cluster in a handful of countries and a few research teams, some with industry ties to the very products being tested. That does not make the work fraudulent. It does mean the picture is narrower and shakier than a confident product label suggests.
Probiotics earn a small, real role as an antifungal sidekick for short-term recurrence, and that is the most the evidence can honestly carry.
Does an oral probiotic even reach where it is supposed to work?
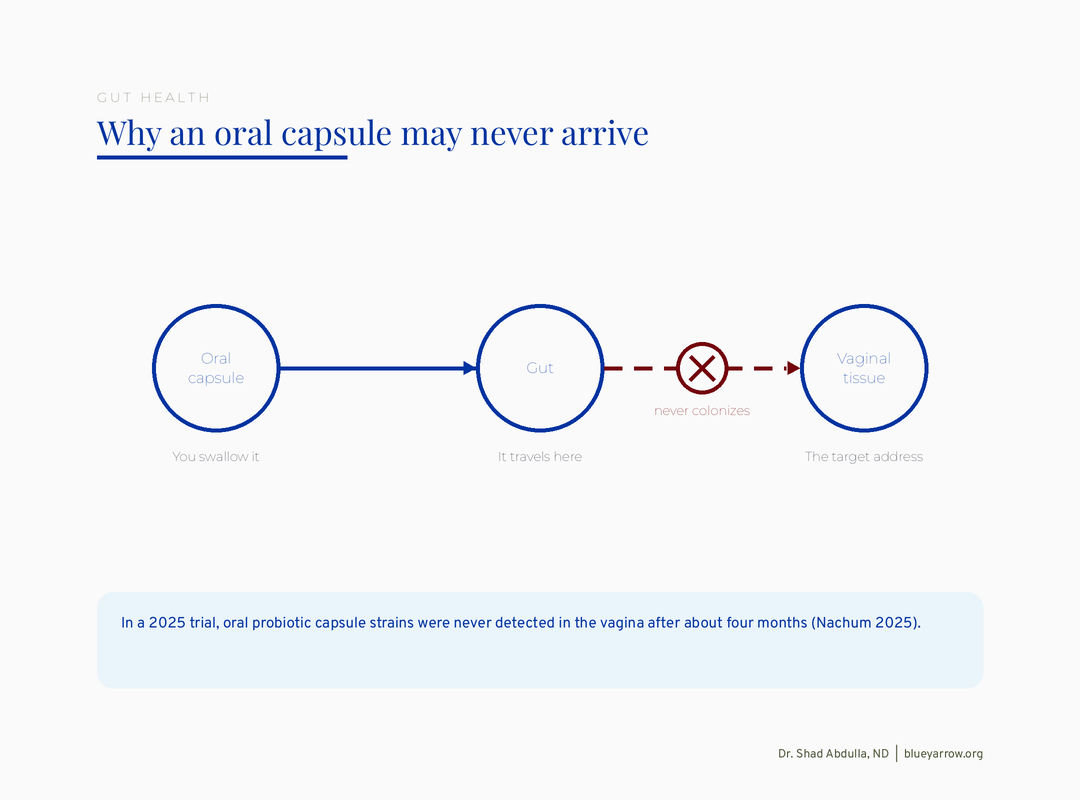
Often, no. This is the part the supplement aisle never mentions, and it is the most important mechanical fact in the whole topic. A capsule you swallow has to somehow get its bacteria from your gut to your vaginal tissue, and the best recent data suggest that frequently does not happen.
In a 2025 trial, researchers gave women oral probiotic capsules and then checked whether those exact strains showed up in the vagina. After four months, they never did (Nachum 2025). The bacteria you paid for never arrived at the address on the label.
Oral probiotic capsules never reached the vagina after four months in a 2025 trial (Nachum).
And even when strains are placed vaginally and do colonize, cure does not reliably follow. One study found that lactobacilli colonized in most women, yet colonization did not predict whether the infection resolved (Marcotte 2019). So the chain the marketing depends on, swallow the capsule, seed the vagina, fix the yeast, breaks at more than one link.
This is the same lesson that runs through so much of probiotic science: the strain and the route matter enormously, and “probiotics” as a single category is far too coarse to mean anything. I went deep on that idea in Why Your Probiotic Isn’t Working (And Which One Might), because it applies to nearly every probiotic decision, not just this one.
A pill that never reaches the tissue it is sold to help cannot do the job the label implies.
Is it even yeast? The question to ask before anything else
Before you reach for a probiotic, or even another antifungal, the single most useful move is to make sure you are treating the right thing. Recurrent symptoms that a woman calls “yeast” are frequently something else, and chasing the wrong diagnosis is why nothing holds.
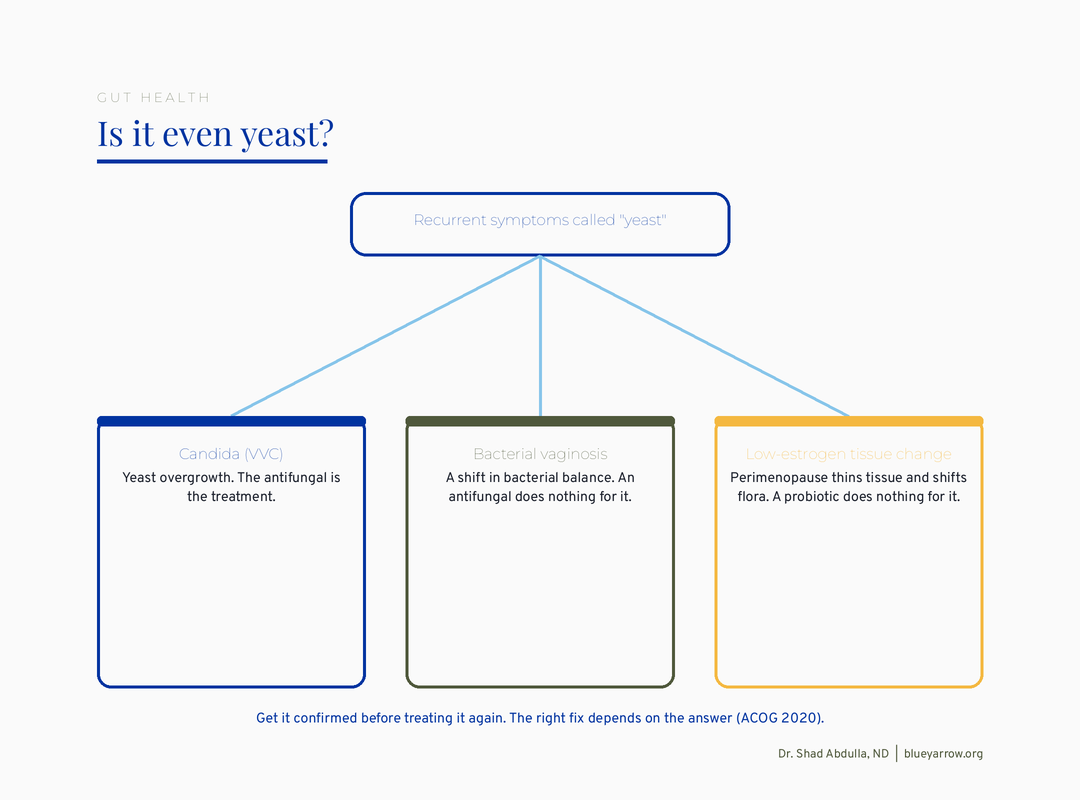
What gets mistaken for yeast? Bacterial vaginosis, a shift in the normal bacterial balance, presents with itching and discharge and gets self-treated as yeast all the time. Plain irritation from soaps, products, or friction can mimic it. And in your early forties, low-estrogen tissue change is a big one. As estrogen declines in perimenopause, the vaginal tissue thins and the normal flora shifts, which can produce irritation, dryness, and discomfort that feels exactly like a yeast infection but is not (ACOG 2020).
This matters because the fix is completely different. An antifungal does nothing for bacterial vaginosis. A probiotic does nothing for thinning, estrogen-starved tissue. If you are 41 to 45 and your “yeast” keeps returning, especially right after your period or after sex, the estrogen-and-flora connection is worth understanding. I mapped that out in The Estrogen-Gut-Vascular Axis in Perimenopause, because the same hormonal shift quietly reshapes more than one system at once.
I am not telling you what you have. I cannot, and no honest article can. I am telling you to get it confirmed before you keep treating it, because a correct diagnosis is the difference between relief and another year of guessing.
If recurrent “yeast” recurs right after your period or arrives new in your forties, get it confirmed before you treat it again.
The wider toolkit, honestly: what naturopathic medicine actually offers here
This is the part the probiotics-only conversation skips, and it is the part I care about most as a naturopathic doctor. There are real options beyond the antifungal, and they are not all the same. Some have randomized trials behind them. Some have centuries of traditional use and early lab work but not the clinical proof yet. And a couple are popular online but genuinely not worth your time or your tissue. I will tell you which is which, plainly, because honest tiering respects you and this medicine more than either hype or dismissal does.
The options with real trials behind them
Boric acid. For stubborn infections, especially azole-resistant ones or those caused by non-albicans Candida species, a 600mg boric acid vaginal suppository is one of the best-supported tools in the whole space. A review of 14 studies reported mycologic cure from 40 to 100 percent (Iavazzo 2011). This is evidence, not folklore. The safety lines are not optional, though. It is a vaginal suppository only, never swallowed, it is toxic and can be fatal by mouth, and it is never used in pregnancy. Keep it away from children, and use it with a clinician’s guidance.
Calendula, a plant I keep coming back to. In a triple-blind trial of 150 women, a Calendula officinalis vaginal cream worked a little slower than clotrimazole at first, then pulled ahead by the second follow-up, with more women testing clear at 30 to 35 days, 77 percent versus 34 percent (Saffari 2016). That is a real randomized result for a traditional botanical, and calendula has a long history in women’s medicine for exactly this kind of raw, inflamed tissue. It is not the emergency treatment for an acute flare, but it is a legitimate, evidence-supported option, and I have deep respect for how this plant works on tissue.
Vaginal probiotics, the route that actually reaches the tissue. Earlier I told you the honest truth that a swallowed capsule often never arrives. Placed vaginally is a different story. In a maintenance trial, a Lactobacillus blend with lactoferrin used as an add-on after the antifungal cut six-month recurrence sharply, to about 29 percent versus 100 percent on placebo (Russo 2019), and a separate randomized trial found vaginal probiotic capsules lowered symptoms and raised the protective lactobacilli (Mandar 2023). The lesson is the one I keep repeating: route and strain are everything. Vaginal, as an add-on for recurrence, is where the real signal lives.
The options with promising mechanism and tradition, but not the clinical proof yet
Tea tree oil and berberine. Both are genuinely interesting, and I will not pretend they are proven cures. In the lab, tea tree oil inhibits Candida, including fluconazole-resistant strains (Ergin 2002; Hammer 2000), and berberine, the bright-yellow compound in goldenseal and barberry, blocks Candida from sticking to vaginal cells (Zhao 2022). That is real mechanism plus long traditional use, the kind documented in the eclectic and phytotherapy literature I trained on. What is missing is the human trial. And tea tree oil can irritate or sensitize vaginal tissue, so it is not something to improvise undiluted. I would call these traditionally used and mechanistically plausible, not established, and I would want a clinician involved before you try them.
The two I would set down
Cutting all sugar to “starve the yeast.” This idea is everywhere and the mechanism sounds reasonable, but no randomized trial supports the anti-Candida diet as a treatment or a prevention for vaginal yeast infections. I am not dismissing food as medicine; I use it constantly. I am telling you this specific claim has outrun its evidence, and I would rather you not spend months on a restriction the trials do not back when better-supported options exist.
Inserting a raw garlic clove. This one I will steer you away from for a concrete reason. There is no clinical support for it, and raw garlic can chemically burn delicate vaginal tissue. Tradition has handed us a great deal that holds up, and part of honoring that tradition is being honest about the few practices that do not. This is one of them.
The wider toolkit is real and worth knowing: boric acid, calendula, and vaginal probiotics have actual randomized trials; tea tree and berberine carry mechanism and tradition but not human proof yet; the all-sugar fast and the raw garlic clove are the two I would set down.
What I’d do this week
This is the part to save. It is a decision guide for the most common situations, so you can find your row and know the honest move. It is education, not a diagnosis.

If I had to compress all of it into one move for this week, it would be this. If you are stuck in the recurrence loop, the first step is not a better probiotic. It is getting the diagnosis right, because the whole approach changes depending on the answer.
Frequently asked questions
Can probiotics cure a yeast infection on their own?
No. The research does not support probiotics as a standalone cure. On the hardest measure, the actual culture result, they perform no better than placebo, and they are inferior to antifungals for lasting cure (Chen 2026). The antifungal is what clears an active infection.
Do probiotics help prevent yeast infections from coming back?
There is a weak signal that adding a probiotic to an antifungal lowers one-month recurrence, but it is low certainty and the benefit does not appear to last (Xie 2017). It is a modest sidekick at best, not a reliable prevention strategy you can count on.
Should I take an oral probiotic or a vaginal one for yeast?
The honest answer is that an oral capsule often never reaches the vaginal tissue at all (Nachum 2025). Vaginal strains colonize more reliably, but even colonization does not guarantee the infection clears (Marcotte 2019). Neither route is proven to cure, so route is a secondary question.
Why do my yeast infections keep coming back?
Sometimes the recurring symptom is not yeast at all. Bacterial vaginosis, irritation, and low-estrogen tissue change in perimenopause all mimic it (ACOG 2020). Recurrence that returns right after your period or arrives new in your forties is worth getting confirmed before you treat it again.
Is boric acid safe for yeast infections?
Used as a vaginal suppository for resistant or non-albicans infections, boric acid has real support, with mycologic cure reported widely across studies (Iavazzo 2011). But it must never be swallowed, it is fatal by mouth, and it must never be used in pregnancy. Use it only with clinical guidance.
Are there naturopathic options that actually work, or is it all unproven?
Several have real randomized trials, and it is a disservice to lump them together. A Calendula officinalis vaginal cream matched and then outperformed clotrimazole for longer-term cure in a triple-blind trial of 150 women (Saffari 2016). Vaginal Lactobacillus with lactoferrin, used as add-on maintenance after the antifungal, cut six-month recurrence to about 29 percent versus 100 percent on placebo (Russo 2019). Boric acid is well supported for resistant cases (Iavazzo 2011). Tea tree oil and berberine show antifungal activity in the lab and have long traditional use, but no human trials yet, so I would treat them as promising rather than proven. The honest move is to tier them, not to wave the whole field away.
Does cutting sugar cure a yeast infection?
No randomized trial supports the anti-Candida diet as a treatment or prevention for vaginal yeast infections. The idea is reasonable-sounding and traditional, but it is not proven, and I would not want you to rely on it in place of getting an accurate diagnosis and appropriate care.
One question for you
If you have come this far, thank you. Here is my question. When your symptoms kept coming back, did anyone ever stop to confirm whether it was actually yeast, or did each visit just hand you another antifungal? Tell me, because the answer shapes what I cover next.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Chen, R., Qing, W., Xu, N., et al. (2026). Probiotics for the treatment of vulvovaginal candidiasis in nonpregnant women: a systematic review and meta-analysis of randomized controlled trials. American Journal of Obstetrics and Gynecology, 234(6), 1604-1622. https://doi.org/10.1016/j.ajog.2026.01.009
2. Xie, H. Y., Feng, D., Wei, D. M., et al. (2017). Probiotics for vulvovaginal candidiasis in non-pregnant women. Cochrane Database of Systematic Reviews, (11), CD010496. https://doi.org/10.1002/14651858.CD010496.pub2
3. Abavisani, M., Sahebi, S., Dadgar, F., et al. (2024). The role of probiotics as adjunct treatment in the prevention and management of gynecological infections: an updated meta-analysis of 35 RCTs. Taiwanese Journal of Obstetrics & Gynecology, 63(3), 357-368. https://doi.org/10.1016/j.tjog.2024.03.004
4. Zahedifard, T., Khadivzadeh, T., & Rakhshkhorshid, M. (2023). The role of probiotics in the treatment of vulvovaginal candidiasis: a systematic review and meta-analysis. Ethiopian Journal of Health Sciences, 33(5). https://doi.org/10.4314/ejhs.v33i5.18
5. Nachum, Z., Suleiman, A., Colodner, R., et al. (2025). Oral probiotics to prevent recurrent vulvovaginal infections during pregnancy. Nutrients, 17(3), 460. https://doi.org/10.3390/nu17030460
6. Liu, Z., Huang, R., Sun, T., & Zhu, L. (2026). Probiotic supplementation during pregnancy for vaginal microbiota improvement and pathogen clearance. Acta Obstetricia et Gynecologica Scandinavica. https://doi.org/10.1111/aogs.70234
7. Marcotte, H., et al. (2019). Pilot study on vaginal lactobacilli administration in women. BMC Infectious Diseases, 19, 824. https://doi.org/10.1186/s12879-019-4425-1
8. Cheng, K. O., Montano, D. E., Zelante, T., Dietschmann, A., & Gresnigt, M. S. (2024). Inflammatory cytokine signalling in vulvovaginal candidiasis. Oxford Open Immunology. https://doi.org/10.1093/oxfimm/iqae010
9. Willems, H. M. E., Lowes, D. J., Barker, K. S., Palmer, G. E., & Peters, B. M. (2018). Comparative analysis of the capacity of Candida species to elicit vaginal immunopathology. Infection and Immunity, 86(12). https://doi.org/10.1128/IAI.00527-18
10. Iavazzo, C., et al. (2011). Boric acid for recurrent vulvovaginal candidiasis. Journal of Women’s Health, 20(8). https://doi.org/10.1089/jwh.2010.2708
11. ACOG. (2020). Vaginitis in Nonpregnant Patients. Practice Bulletin 215. Obstetrics & Gynecology. PMID 32332401
12. CDC. (2021). Sexually Transmitted Infections Treatment Guidelines: Vulvovaginal Candidiasis. https://www.cdc.gov/std/treatment-guidelines/candidiasis.htm
13. Saffari, E., Mohammad-Alizadeh-Charandabi, S., Adibpour, M., et al. (2016). Comparing the effects of Calendula officinalis and clotrimazole on vaginal Candidiasis: A randomized controlled trial. Women & Health, 57(10), 1145-1160. https://doi.org/10.1080/03630242.2016.1263272
14. Russo, R., Superti, F., Karadja, E., & De Seta, F. (2019). Randomised clinical trial in women with Recurrent Vulvovaginal Candidiasis: Efficacy of probiotics and lactoferrin as maintenance treatment. Mycoses, 62(4), 328-335. https://doi.org/10.1111/myc.12883
15. Mändar, R., Sõerunurk, G., Štšepetova, J., et al. (2023). Impact of Lactobacillus crispatus-containing oral and vaginal probiotics on vaginal health: a randomised double-blind placebo controlled clinical trial. Beneficial Microbes, 14(2), 143-152. https://doi.org/10.3920/BM2022.0091
16. Ergin, A., & Arikan, S. (2002). Comparison of microdilution and disc diffusion methods in assessing the in vitro activity of fluconazole and Melaleuca alternifolia (tea tree) oil against vaginal Candida isolates. Journal of Chemotherapy, 14(5), 465-472. https://doi.org/10.1179/joc.2002.14.5.465
17. Hammer, K. A., Carson, C. F., & Riley, T. V. (2000). Melaleuca alternifolia (tea tree) oil inhibits germ tube formation by Candida albicans. Medical Mycology, 38(5), 355-362.
18. Zhao, T., Zhang, K., Shi, G., et al. (2022). Berberine inhibits the adhesion of Candida albicans to vaginal epithelial cells. Frontiers in Pharmacology, 13, 814883. https://doi.org/10.3389/fphar.2022.814883
19. Bone, K., & Mills, S. Principles and Practice of Phytotherapy: Modern Herbal Medicine (tea tree and Berberis/Hydrastis monographs). [Naturopathic textbook, traditional-use and clinical depth.]