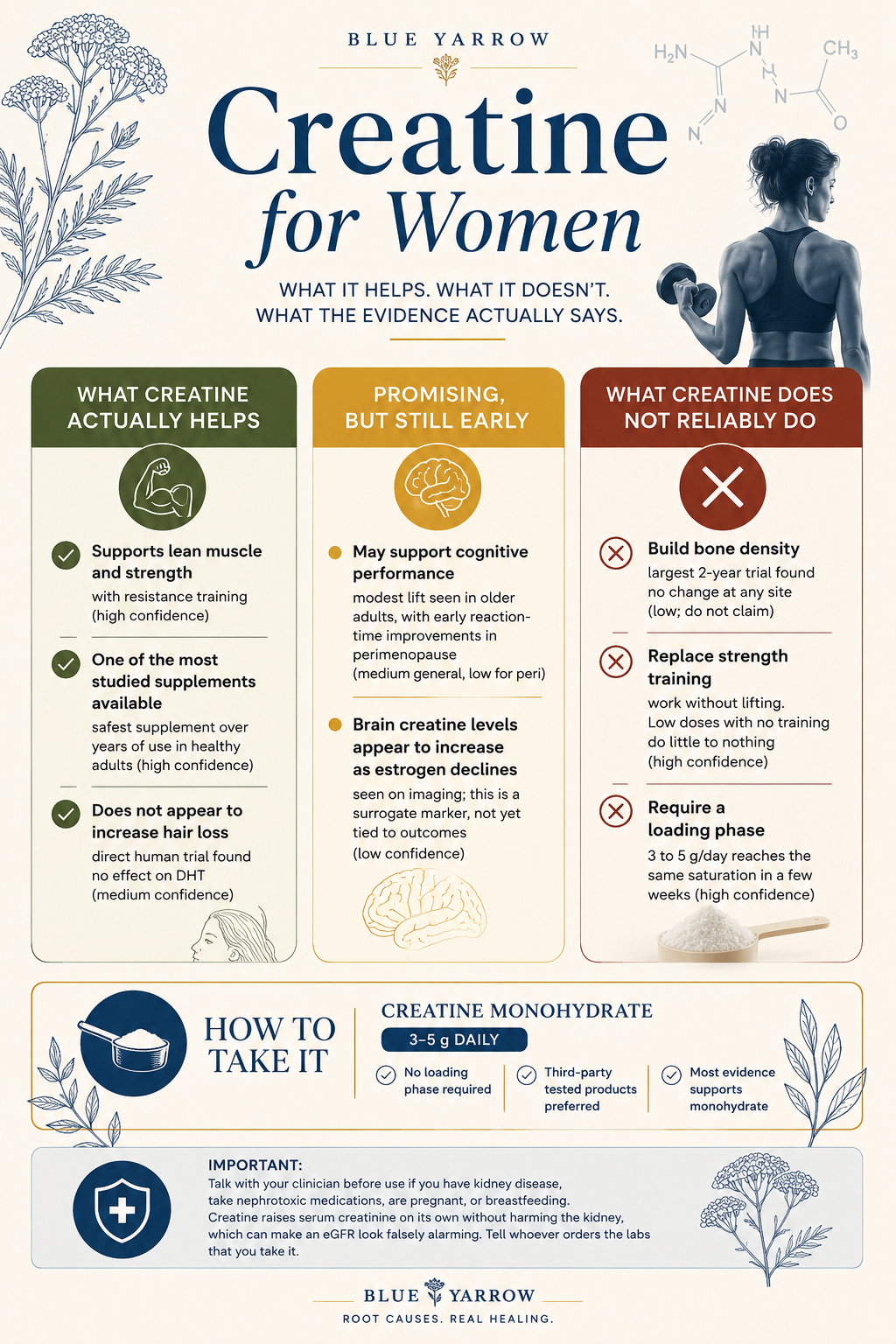
Creatine for Women: What It Does, and What It Doesn’t
If you are in your forties and every reel on your feed is telling you to take creatine, and you are quietly wondering whether it is actually for you or just the next thing you are supposed to buy, this one is for you. I have watched the same scene play out over and over: a woman has read that one scoop will protect her muscle, her bones, her brain, and her mood all at once, and she wants to know if that is true before she spends another $30 on hope. Here is the honest answer, and it is the reason I wanted to write this. The muscle and strength benefit is real and well studied. The perimenopausal brain signal is new and genuinely interesting. The bone-density promise, the one almost everyone leads with, is the weakest of the three and the largest study found nothing. So the question is not really “does creatine work.” It is “which of the three things on the label am I actually buying.” This piece walks through all three, plus the dose, the safety questions you keep asking, and a one-page triage card you can save for later.
One supplement got fused into one promise. The evidence does not split evenly across it. Let me back up and take the three pieces one at a time.
What creatine actually is, and why women are taking it now
Short answer: creatine is a compound your body already makes and stores mostly in muscle, where it helps recycle the energy currency your cells run on. You are not adding a foreign drug. You are topping off a tank you already have.
If you have felt like creatine appeared out of nowhere in women’s wellness over the last two years, you are not imagining it. The data backs up the feeling. Creatine led all 200 supplements ConsumerLab tracks for growth in early 2026, and women are now the demographic driving the surge, up from a small slice of buyers five years ago to nearly a third at one major retailer. The average buyer is no longer a twenty-something man at the gym. She is around 35, often perimenopausal, often someone who feels her body changing and wants something that helps.
Here is the mechanism in plain terms. Creatine and its active form, phosphocreatine (the charged version your cells keep on hand for fast energy), buffer ATP (adenosine triphosphate, the molecule that powers nearly everything your cells do) in tissues with high, swinging energy demand. Muscle is one of those tissues. The brain is another. That single fact is why one supplement got marketed for muscle, bone, and brain at the same time. The biology is shared. The clinical proof is not, and that gap is the whole story.
Creatine is endogenous, well studied, and having a real moment with women over 35. The reason it gets sold for everything at once is that the mechanism touches everything at once. Mechanism is a starting point, not a finish line.
Does creatine build muscle and strength in women? Yes, with lifting
Short answer: yes, but only when you pair it with resistance training. This is the one claim with solid data behind it, and it is the one I would tell any woman to lean on.
You probably want to know what the number actually is, not just “it helps.” Here it is. Creatine plus lifting adds about 7.5 kg to leg-press strength versus training alone (Naddafha 2026 meta-analysis, n=608). That same review found lean mass (the non-fat tissue your metabolism and your independence depend on) rose by a modest amount too. These are not huge effects. They are real, consistent, and low-risk, which in supplement research is rare and worth respecting.
The part the marketing skips: the benefit showed up only when the dose was 5 grams a day or more and it was combined with lifting. Trials that used low doses without training found nothing. Creatine does not build muscle on its own. It amplifies the work you are already doing. Think of it as a slightly better return on every squat, not a shortcut around them.
I will be straight with you about the limit of this evidence, because it matters. Most of these trials were done in postmenopausal women with a mean age near 60. For a 38- or 43-year-old, the muscle benefit is a reasonable extrapolation, but it is less directly proven, and one large strength review (Kazeminasab 2025) found the effect was clearer in men than in women across several measures. The female effect looks real but smaller and less consistent. I would rather you know that than be sold certainty I cannot back.
Strength and lean mass, with lifting, is the high-confidence claim. The honest footnote is that most evidence comes from older women and the female effect may be smaller than the male one. For the woman in front of me carrying groceries up two flights and feeling it more than she used to, this is the part of the label worth her money.
The bone question almost everyone gets wrong
Short answer: creatine does not reliably build bone density, and the largest, longest trial is the reason I say that. The bone promise is the weakest of the three, even though it is the one you hear first.
Let me say the thing I genuinely mean before the correction, because it matters. I love that more women are strength training and taking creatine seriously in midlife. That instinct, to protect muscle and bone before the slope steepens, is exactly right, and the people championing it have moved this conversation forward. Here is the part the excitement is getting ahead of. The largest trial, 237 women over 2 years, found no creatine bone-density benefit at any site (Chilibeck 2023). No change at the hip, the femoral neck, or the spine.
So where did the bone story come from? It is not invented. An earlier, smaller one-year trial in 2015 showed creatine slowed bone loss at the femoral neck, and that signal got quoted everywhere. Then the same research group ran a bigger, longer, lower-bias study, and the BMD (bone mineral density, what a DEXA scan measures) benefit did not hold up. The longer, larger trial wins on evidentiary weight. That is how science is supposed to self-correct, and it is not a knock on anyone to say so.
One nuance worth keeping, because precision is the point. The 2-year trial did preserve bone geometry (the structural shape and strength of the bone, things like section modulus, which is roughly a measure of how well a bone resists bending) even though it did not raise density. So “creatine does nothing for bone” would itself be an overstatement. The accurate statement is narrower: the bone-density claim is overstated and unsettled, and you should not take creatine as your bone strategy.
[ONE-THING-TEST: REPLACE BEFORE PUBLISHING]
AI placeholder (do not ship as-is): “The creatine question women keep asking me is not whether it builds muscle, it is whether the bone and brain promises on the label are real, and most of the time the honest answer is not yet.”
Your turn. Write the line only you could have written. Prompts: - What is the exact moment a 43-year-old asks you about creatine, and what is she really worried about underneath the question? - What did you think about creatine before you read this evidence, and what changed your mind? - What is the one thing the menopause-supplement marketing gets right that you want to protect, before you correct the part it gets wrong? - Where do you see women conflating “I take creatine” with “I am protecting my bones,” and what would you tell them instead?
Constraints: - One sentence, max 25 words - Specific (number, body part, demographic, year) > general - Clinical observation > opinion - Names a pattern, not a fear
[/ONE-THING-TEST]
Geometry was preserved. Density was not. If a woman is tracking her bone, creatine is not the lever; load-bearing strength training, and the things her clinician recommends, are. What I tell women who ask: take creatine for the muscle, and protect your bones with weight, not with a scoop.
The brain and perimenopause signal: promising, but early
Short answer: there is an early, interesting signal that creatine may support the perimenopausal brain, but it rests on one small trial, so I hold it loosely. This is the part I find most genuinely exciting and the part I am most careful about overselling.
If brain fog has been the symptom that scares you most, the word that will not surface mid-sentence, the meeting where you lost the thread, I understand why this claim grabs you. It is the symptom with the fewest good answers. So here is what the evidence actually shows, with the number. Creatine raised frontal brain creatine 16.4% versus 0.9% on placebo in one perimenopausal trial (CONCRET-MENOPA, n=36, 2025). That same small trial also found a faster reaction time on creatine.
Here is why I am cautious. Raising brain creatine on a scan is a surrogate, a stand-in measurement, not the outcome you care about. It is biologically necessary for a cognitive effect, but it is not proof of one. The trial had 36 women. The largest general cognition trial in adults was close to null. And a memory meta-analysis found the clearest benefit in adults aged 66 to 76, not in women in their forties.
The mechanism is the appealing part and also the honest caveat. Estrogen seems to influence how the brain handles creatine, so the perimenopausal transition is hypothesized to leave a brain-energy gap that supplementation might partially fill. That is a compelling story. It is not yet a proven outcome, and I will not call creatine a treatment for brain fog, because it is not one and the evidence cannot carry that weight.
The brain-energy mechanism is strong. The brain-outcome data is thin, on-cohort but tiny, and dose is unsettled. For the woman white-knuckling through perimenopausal fog, this is a reasonable thing to try with eyes open, not a fix to count on.
The dose nobody agrees on, and why you don’t need to load
Short answer: 3 to 5 grams a day of creatine monohydrate, every day, no loading phase required. The strength evidence sits at 5 grams or more paired with lifting.
The loading phase, that week of 20 grams a day split into four doses, is a holdover from 1990s male hypertrophy protocols, and product marketing loves it because it sells more powder. You do not need it. Loading saturates your muscle faster, but a steady 3 to 5 grams a day reaches the same saturation in a few weeks, with fewer of the GI side effects (stomach upset, the bloating people complain about) that loading can cause. Skipping the load is not a compromise. It is the better-tolerated path to the same destination.
On form: choose creatine monohydrate, and choose one that is third-party tested. Look for NSF Certified for Sport or Informed Sport on the label, because creatine is a supplement, not an FDA-pre-approved drug, and quality varies. The newer forms you will see marketed, creatine HCl, ethyl ester, gummies, carry less efficacy evidence than plain monohydrate despite the prettier packaging. Monohydrate is the most studied, the cheapest, and the one I would point anyone toward.
The one genuinely open question is dose for the brain. The strength data is settled at 5 grams. The cognition research has used everything from low doses up to 20 grams, and nobody has nailed down what the brain actually needs, especially in perimenopausal women. So if your goal is muscle and strength, the dose is clear. If your goal is the brain signal, you are in honest experimental territory, and I would say so out loud rather than pretend otherwise.
Three to five grams daily, monohydrate, third-party tested, no loading. The brain dose is the only piece still genuinely up for debate. Keep it simple; the simple version is the one with the evidence.
Is creatine safe? Will it make me bulky? Will I lose my hair?
Short answer: creatine is one of the most studied and safest supplements there is, it will not make you bulky at these doses, and the one trial that looked directly at hair did not find an effect.
These are the three objections I hear most, so let me take them in order. On safety: creatine monohydrate has been studied for years in healthy adults with no consistent harm to the kidneys at normal doses. It is, genuinely, among the most well-characterized supplements on the shelf. The bulk fear is the easiest to retire: the small weight bump some women notice early is water drawn into muscle, not fat, and not the kind of bulk women worry about. You are not going to wake up looking like a bodybuilder from 5 grams a day.
On hair: the fear traces back to a single 2009 study in rugby players that showed a rise in DHT (dihydrotestosterone, an androgen hormone linked to hair thinning) without ever measuring hair. A more recent 12-week trial looked directly at DHT and hair parameters and found no effect. The honest evidence does not support the hair-loss claim, though I will note that trial was in men, so it answers the mechanism question more than the female-specific one.
Now the practical safety notes that actually matter for you. Creatine raises serum creatinine (a blood marker labs use to estimate kidney function) on its own, without harming the kidney. That can make an eGFR (estimated glomerular filtration rate, the calculated number that flags kidney problems) look falsely alarming. So if you have bloodwork coming up, tell whoever orders it that you take creatine. Check with your clinician first if you have kidney disease or take nephrotoxic drugs, and if you are pregnant or breastfeeding, the trials simply have not been run, so the absence of data is not a green light.
Safe in healthy adults, not bulky, not a proven hair-loss culprit, with two real cautions: tell your lab, and clear it first if you have kidney concerns or are pregnant. What this means for the woman in front of me is that the safety story is reassuring but not a blank check, and the lab note alone is worth the price of reading this.
What I’d do this week
If you take one thing from all of this, take the triage below. Save it, screenshot it, send it to the friend who just bought her first tub. It is the honest cheat sheet I wish more women had before they spent the money.
The creatine triage card
The one-week version: if you lift, add 5 grams of monohydrate a day and skip the loading nonsense. If you do not lift yet, start there first; the powder follows the work, not the other way around.
The honest bottom line
Creatine is not the all-in-one women’s supplement the feed is selling, and it is not a scam either. It is a precise tool. For muscle and lower-body strength, paired with lifting, it has earned its place and I would tell almost any midlife woman it is reasonable. For the perimenopausal brain, it is a promising early signal worth trying with clear eyes, not a fix to bank on. For bone density, it is the wrong lever, and the strongest evidence says so plainly.
The reason I wanted to write this is that you deserve to know which of the three you are actually buying, instead of paying for one promise and receiving a different one. Take it for the muscle. Stay curious about the brain. Protect your bones with weight, not powder.
So here is my question for you: when you started, or thought about starting creatine, which of the three was the real reason, and does that reason match the evidence you just read? That answer tells you whether to keep going, change how you use it, or spend the money somewhere it works harder.
Frequently asked questions
Is creatine safe for women to take long-term? For healthy women, the evidence is reassuring. Creatine monohydrate has been studied for years with no consistent kidney harm at normal doses. The honest limit is that very long-term data specifically in women across the menopausal transition does not yet exist, so “well tolerated” is accurate while “studied for decades in your exact group” is not.
Will creatine make me gain weight or look bulky? Not in the way women usually fear. Any early weight bump is water drawn into muscle, not fat, and 3 to 5 grams a day does not produce the bulk associated with heavy training plus a calorie surplus. You may notice a pound or two of water early on. That is the saturation working, not your body changing shape.
Do I have to do a loading phase? No. Loading, 20 grams a day for a week, saturates your muscle faster but is not required and tends to cause more stomach upset. A steady 3 to 5 grams daily reaches the same saturation in a few weeks. The loading phase is a holdover from older male training protocols, not a necessity for women.
Does creatine actually help with perimenopausal brain fog? The signal is early and I would not call it a treatment. One small 2025 trial in perimenopausal women raised brain creatine and improved reaction time, which is interesting but rests on 36 women and a surrogate marker. The mechanism is plausible, the outcome data is thin, and the right dose for the brain is still unsettled.
Does creatine build bone or prevent osteoporosis? The strongest evidence says it does not reliably build bone density. The largest trial, 237 women over two years, found no change at any site, although it did preserve bone geometry. If bone is your concern, weight-bearing strength training and your clinician’s guidance are the levers, not creatine.
Does creatine cause hair loss? The trial that looked directly at hair did not find an effect. A 12-week study measuring DHT and hair parameters found nothing. The hair-loss fear traces to a single 2009 study that showed a DHT rise but never measured hair. That trial was in men, so it answers the mechanism more than the female-specific question, but it does not support the claim.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. Naddafha, S., Antonio, J., Kreider, R. B., & Stout, J. R. (2026). Creatine monohydrate for lean mass, strength, and bone density in postmenopausal women: A systematic review and meta-analysis. Journal of the International Society of Sports Nutrition, 23(1), 2668435. https://doi.org/10.1080/15502783.2026.2668435
2. Kazeminasab, F., Kerchi, A. B., Sharafifard, F., Forbes, S. C., Bagheri, R., et al. (2025). The effects of creatine supplementation on upper- and lower-body strength and power: A systematic review and meta-analysis. Nutrients, 17(17), 2748. https://doi.org/10.3390/nu17172748
3. Chilibeck, P. D., Candow, D. G., Gordon, J. J., Duff, W. R. D., Mason, R., Shaw, K., et al. (2023). A 2-yr randomized controlled trial on creatine supplementation during exercise for postmenopausal bone health. Medicine and Science in Sports and Exercise, 55(10), 1750-1760. https://doi.org/10.1249/MSS.0000000000003202
4. Chilibeck, P. D., Candow, D. G., Landeryou, T., Kaviani, M., & Paus-Jenssen, L. (2015). Effects of creatine and resistance training on bone health in postmenopausal women. Medicine and Science in Sports and Exercise, 47(8), 1587-1595. https://doi.org/10.1249/MSS.0000000000000571
5. Korovljev, D., Ostojic, J., Panic, J., Ranisavljev, M., Todorovic, N., et al. (2025). The effects of 8-week creatine hydrochloride and creatine ethyl ester supplementation on cognition, clinical outcomes, and brain creatine levels in perimenopausal and menopausal women (CONCRET-MENOPA): A randomized controlled trial. Journal of the American Nutrition Association, 45(3), 199-210. https://doi.org/10.1080/27697061.2025.2551184
6. Prokopidis, K., Giannos, P., Triantafyllidis, K. K., Kechagias, K. S., Forbes, S. C., & Candow, D. G. (2023). Effects of creatine supplementation on memory in healthy individuals: A systematic review and meta-analysis of randomized controlled trials. Nutrition Reviews, 81(4), 416-427. https://doi.org/10.1093/nutrit/nuac064
7. Sandkuhler, J. F., Kersting, X., Faust, A., Konigs, E. K., et al. (2023). The effects of creatine supplementation on cognitive performance: A randomised controlled study. BMC Medicine, 21(1), 440. https://doi.org/10.1186/s12916-023-03146-5
8. Lak, M., Forbes, S. C., Ashtary-Larky, D., et al. (2025). Does creatine cause hair loss? A 12-week randomized controlled trial. Journal of the International Society of Sports Nutrition, 22(sup1), 2495229. https://doi.org/10.1080/15502783.2025.2495229
9. Lobo, D. M., Tritto, A. C., da Silva, L. R., de Oliveira, P. B., Benatti, F. B., et al. (2015). Effects of long-term low-dose dietary creatine supplementation in older women. Experimental Gerontology, 70, 97-104. https://doi.org/10.1016/j.exger.2015.07.012
10. Kreider, R. B., Kalman, D. S., Antonio, J., Ziegenfuss, T. N., Wildman, R., et al. (2017). International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14, 18. https://doi.org/10.1186/s12970-017-0173-z
11. Chilibeck, P. D., Kaviani, M., Candow, D. G., & Zello, G. A. (2017). Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: A meta-analysis. Open Access Journal of Sports Medicine, 8, 213-226. https://doi.org/10.2147/OAJSM.S123529
12. Smith-Ryan, A. E., DelBiondo, G. M., Brown, A. F., Kleiner, S. M., Tran, N. T., & Ellery, S. J. (2025). Creatine in women’s health: Bridging the gap from menstruation through pregnancy to menopause. Journal of the International Society of Sports Nutrition, 22(1), 2502094. https://doi.org/10.1080/15502783.2025.2502094