What Your AMH Result Actually Means (Updated May 2026)
If you have ever opened a Modern Fertility email with a low AMH (anti-Mullerian hormone, a blood marker made by small growing follicles in the ovary) result and felt the floor drop, this post is for you. If your doctor said “the number does not matter unless you are trying to conceive” and you walked out feeling unseen, this is for you too. I have read the literature on ovarian age testing closely, and the honest answer sits in a quieter middle than either side of your feed is telling you. Your AMH is a useful number inside a narrow set of clinical scenarios. It is not your longevity score. It is not a verdict on your fertility timeline. And it does carry a real population-level cardiometabolic signal that deserves respect, not panic. Below I walk through what the test actually measures, what the strongest published studies say about predicting fertility and menopause, where the heart-health signal does live, how oral contraception changes the number, and the four questions to ask before you make any decision based on a single result.
What is AMH and what does the test actually measure?
If you have been told AMH is your “egg count,” that is the shorthand that sells the test, and it is not what the biology shows. AMH (anti-Mullerian hormone) is a protein made by granulosa cells inside small growing follicles in the ovary, specifically the preantral and small antral follicles. It reflects the size of the growing follicle pool at any moment in time. Your total reserve of dormant eggs (the primordial follicle pool, the eggs you were born with) is not directly measured by any clinical blood test currently available.
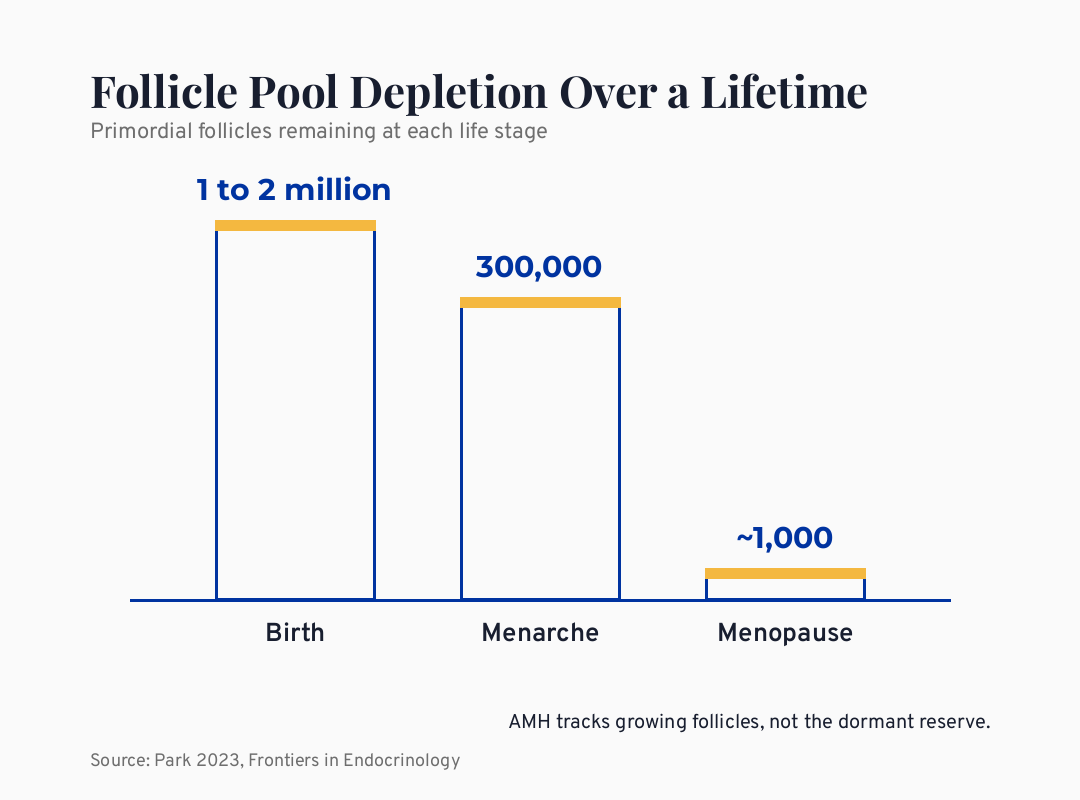
Here is the scale. A baby girl is born with roughly 1 to 2 million primordial follicles. By the time she menstruates, the count is around 300,000. The decline accelerates after the mid-30s, and by menopause, roughly 1,000 follicles remain (Park 2023, Frontiers in Endocrinology). Monthly recruitment of growing follicles also drops, from 800 to 900 per cycle at menarche to fewer than 100 near menopause. AMH tracks the recruited pool, not the dormant one. That is an important difference, because the marker the consumer market sells as your egg counter is in fact a snapshot of follicular activity, which is shaped by biology, hormonal context, and the natural depletion curve of ovarian aging.
The short version: AMH is the best blood proxy currently available for ovarian reserve, but it measures the small growing follicles, not your total egg supply, and that distinction changes how a single result should be read.
What does my AMH actually predict about my chances of getting pregnant?
If you are in your thirties or early forties and trying to conceive naturally, this is the single most important number to put in front of your low AMH result. Steiner 2017 (n=750) found women under 44 with low AMH had the same natural conception odds as women with normal AMH. The study, published in JAMA, followed 750 women with a mean age of 33.3 attempting to conceive over 6 and 12 cycles. Low AMH (under 0.7 ng/mL) and high FSH (follicle-stimulating hormone, the pituitary hormone that drives follicle recruitment) did not lower the probability of conception. The authors concluded directly that AMH and urinary or blood FSH should not be used to assess natural fertility in women in this age range.
A woman I worked with several years ago, anonymized here, had ordered a DTC (direct-to-consumer) AMH test at 34 out of curiosity and received a number lower than the age-stratified reference range. She spent six weeks crying about it before she came across this paper. She conceived naturally the following year, on her own timeline, without intervention. The number on her report had not predicted her cycle. It had predicted her panic.
The point is not that AMH means nothing. It is that AMH is a marker built and validated for predicting how an ovary responds to IVF stimulation, not for predicting whether a woman with otherwise normal cycles will conceive naturally in the next twelve months. The ASRM (American Society for Reproductive Medicine) Practice Committee opinion is explicit: ovarian reserve testing should serve as an adjunct to the evaluation of infertile women, not as a screening test for women not meeting infertility criteria.
When I read this paper, I think about every woman who paid $159 for a Modern Fertility kit and received a number that did not change a single fertility outcome but did change how she felt in her own body for months. That is the gap doctor-grade content is supposed to close.
Will my AMH tell me when I will go through menopause?
This is the second-most common question I see in the audience, and the honest answer takes some unpacking. AMH adds 2 percentage points of predictive accuracy over age alone for menopause timing (Depmann 2018 IPD meta-analysis, n>5,000). That is from an individual patient data meta-analysis published in the Journal of Clinical Endocrinology and Metabolism in 2018. The model accuracy (C-statistic) moves from 84% with age alone to 86% with age plus AMH. That is a real but small improvement, and the prediction interval for any individual woman remains wide, especially at the extremes of the distribution.
Here is what that means for the woman in front of me. If you are 33 and your AMH is “low for your age,” the model still cannot tell you whether you will reach menopause at 47 or at 53. The confidence interval around the prediction is too wide for that level of personal planning. The marketing claim that AMH is an “egg timer” trades on a metaphor the biology does not support at the individual level.
There is one important exception. In late-reproductive women, the picture sharpens. The SWAN study sub-analysis (Finkelstein 2020, n=1,537) showed that an ultrasensitive AMH less than 10 pg/mL in women aged 42 to 53 has a 78 to 97% positive predictive value for the final menstrual period within three years. That is a meaningful clinical signal for a woman in her early forties who is trying to plan around perimenopause. It does not translate down into a 33-year-old’s life.
The short version: AMH offers a tiny prediction bump over age alone for general-population menopause timing, and the prediction sharpens only in women 42 and up with very low AMH on an ultrasensitive assay.
Why do ACOG and ASRM both recommend against general-population AMH screening?
Because the prediction at the individual level is not strong enough to justify the downstream anxiety, intervention, and cost the testing generates. ACOG (American College of Obstetricians and Gynecologists) Committee Opinion No. 773 from 2019 states directly that using AMH for fertility counseling in women without a diagnosis of infertility “is not currently supported by data from high-quality sources.” The newest guidance, ACOG Committee Statement No. 22 from November 2025, reinforces that position and adds a call for clinician-led anticipatory counseling rather than DTC testing in women who are not pursuing fertility care. NICE (the UK National Institute for Health and Care Excellence) and the ASRM Practice Committee say the same.
These bodies are not denying that women want information. They are saying that a single AMH value in a healthy 33-year-old does not reliably guide a fertility decision and can drive a cascade of testing, treatment, and elective procedures that the evidence does not support. The international PCOS guideline updated in 2023 does accept AMH as an alternative to ultrasound for the polycystic ovarian morphology criterion in PCOS (polycystic ovary syndrome) diagnosis, but that is a specific diagnostic context, not a screening context.
Here is the lived experience underneath that guideline. A woman who orders a DTC AMH test out of curiosity, receives a low result, and walks into her primary care office often gets one of two responses. Either the doctor dismisses the test entirely (“ignore it, you are fine”), or the doctor refers her to a fertility clinic where the conversation tilts toward early intervention. Neither response includes a thirty-minute conversation about what the number actually predicts and what it does not. The guideline exists because the gap between the test and the meaningful counseling around it has been very wide.
Is there a real connection between ovarian aging and heart health?
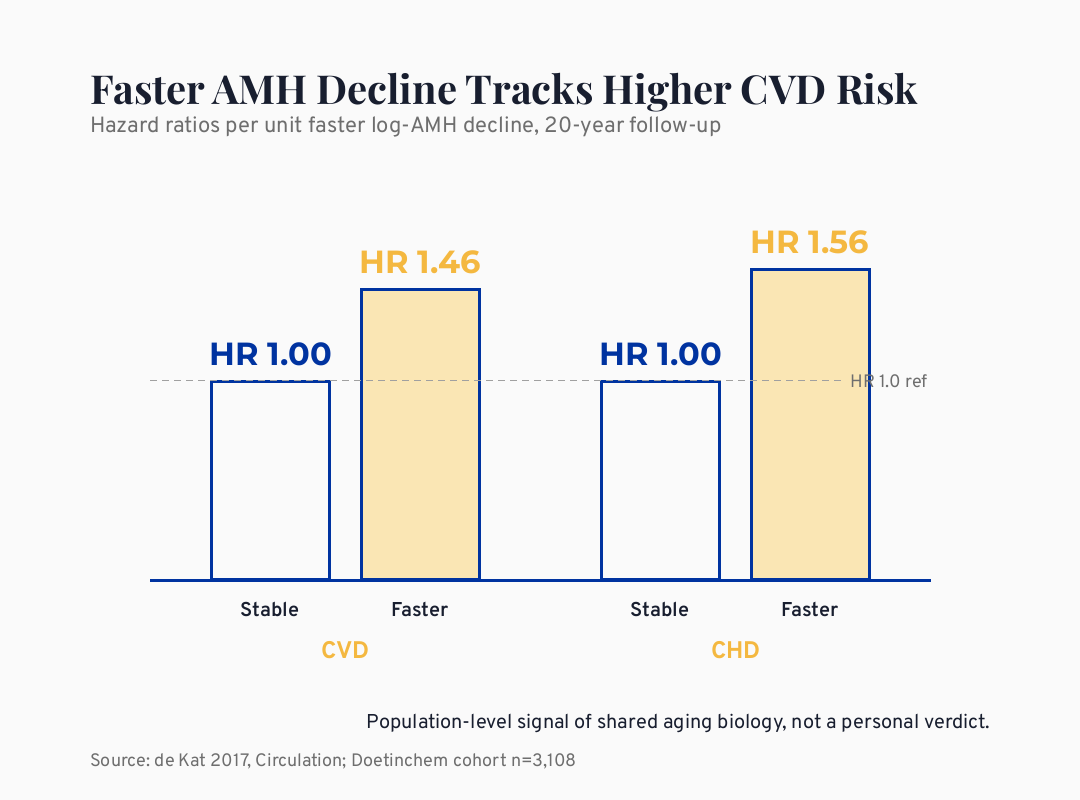
Yes, and this is the part of the literature that almost no one in the consumer space is talking about. Per unit faster log-AMH decline, CVD risk rose 46% over 20 years versus stable-AMH peers (de Kat 2017, Doetinchem n=3,108). The Doetinchem cohort, published in Circulation, followed more than 3,000 Dutch women for two decades with serial AMH measurements. Faster log-AMH decline was independently associated with a 46% higher cardiovascular disease (CVD) incidence and a 56% higher coronary heart disease (CHD) incidence. That is a hazard ratio in the range usually reserved for established cardiovascular risk factors.
The authors are careful with the causal claim. Declining AMH is not thought to cause heart disease directly. The hypothesis is that ovarian aging and vascular aging share an underlying biology of oxidative stress, mitochondrial damage, and inflammatory milieu changes. The ovary may simply be one of the most sensitive readouts of a system-wide aging process. A separate body of evidence, including a Lancet Public Health 2019 pooled analysis and a JAMA Cardiology 2016 meta-analysis, links earlier age at natural menopause to higher all-cause and cardiovascular mortality. The signal lines up across study designs.
I want to be careful here. The Doetinchem signal is the strongest cardiometabolic data on AMH trajectory in the published literature, and it is concentrated in a single Dutch cohort. Independent replication in Black, Hispanic, South Asian, and Middle Eastern populations is still limited, and AMH age-specific reference ranges differ meaningfully by ethnicity. This is a population-level signal worth taking seriously for risk awareness, not a personal verdict that any individual woman with declining AMH is destined for a cardiac event. The honest framing is that the trajectory is worth knowing, and the leverage you have over cardiovascular risk through sleep, strength training, blood pressure, blood glucose, ApoB (apolipoprotein B, a lipid marker that tracks atherogenic particle count better than LDL alone), and visceral adiposity is enormous compared to the leverage you have over your AMH number itself.
The short version: the AMH-and-cardiovascular link is a real, replicated, population-level signal that the femtech market downplays and the conventional system rarely names; it is a reason to take ovarian-age data seriously without making it the only number on the page.
How do birth control pills change my AMH result?
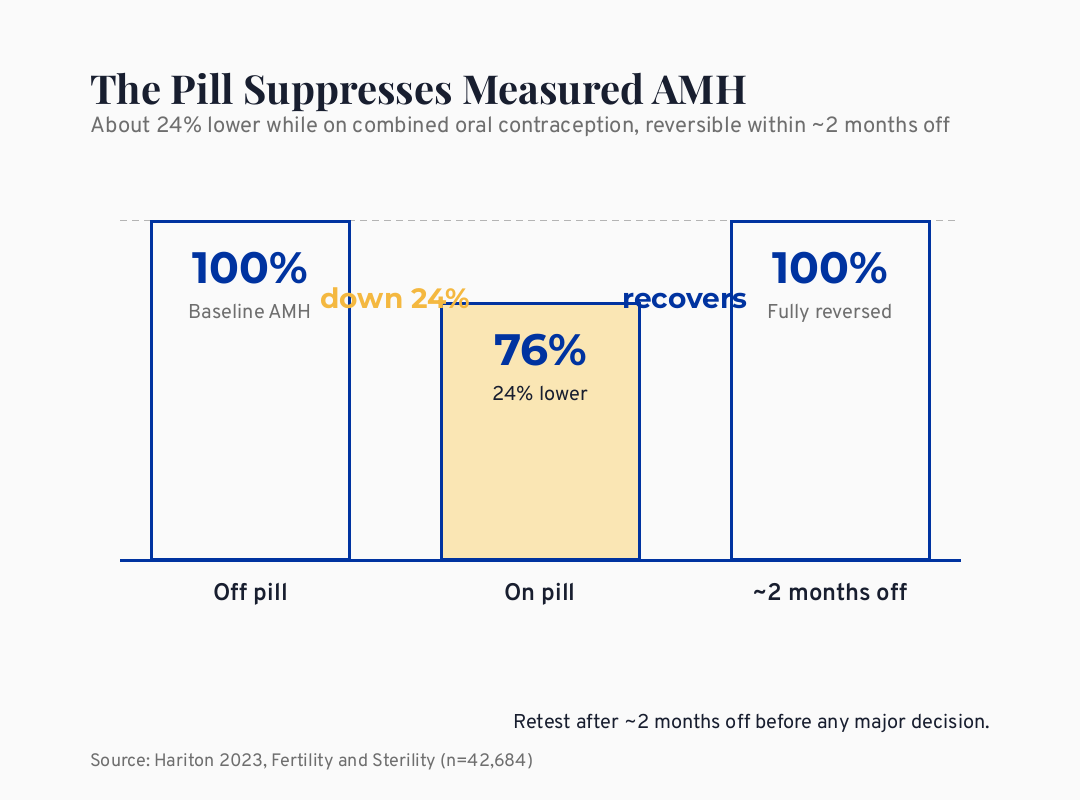
This is the single most under-counseled point in DTC test reporting. Combined oral contraceptive (COC) use suppresses measured AMH by approximately 24%, fully reversible within roughly two months of discontinuation, in a Hariton 2023 study of 42,684 women published in Fertility and Sterility. If you were on the pill when your AMH was drawn and the result came back lower than the age-stratified reference range, the most honest interpretation is retest after washout before you allow that number to drive any decision about your reproductive future. GnRH agonists (gonadotropin-releasing hormone agonists, a drug class that suppresses ovarian function), recent ovarian surgery, and active chemotherapy all suppress the result as well.
I have seen this pattern in cases I have reviewed more than once. A woman in her early thirties on the pill orders a DTC test, sees a number that triggers her, and starts pricing egg-freezing cycles within the week. The result she is panicking over may overstate her ovarian-reserve decline by a quarter. The retest after washout is the boring, unmonetized step the test report rarely emphasizes.
What this means for the woman holding a low result: before you make any decision that costs you money, time, or your peace of mind, confirm the contraceptive context of the draw and consider repeating the test after roughly two months off hormonal contraception. The number that drives a decision should be drawn under conditions that let you trust it.
What about the longevity industry’s “ovaries as master clock” claim?
The claim that ovarian aging is the master clock of female biological aging is industry narrative, not Tier 1 evidence. It is the candidate story the longevity sector needs to differentiate from a male-default biological-aging market that is built around testosterone, frailty, and prostate health. Hevolution, Oviva Therapeutics (acquired by Granata Bio in 2025), Gameto, the VIBRANT rapamycin trial at Columbia, and a planned 2026 XPRIZE on ovarian function are all moving real capital into ovarian-aging research. That investment will eventually generate the evidence base the consumer claim has been making ahead of.
For now, the master-clock framing rests on the shared-aging-biology hypothesis (real, partially supported by the de Kat data) and on industry-funded preclinical and early clinical work (legitimate science, early stage). The VIBRANT trial early signal, often summarized in the press as “20% slower ovarian aging” and translated further into “five more fertile years,” is from a small RCT (randomized controlled trial) whose full primary publication is still pending. VIBRANT II is planned at n=1,000 and will be a much more meaningful read on whether weekly rapamycin meaningfully delays ovarian-reserve decline in healthy women.
Here is the honest stance. I find the ovarian-aging research direction genuinely interesting and I am following it closely. I am not yet at “take rapamycin to delay menopause” as a thing I would tell anyone who asks. That recommendation requires safety data that does not yet exist in healthy reproductive-age women, and the drug carries known immunosuppressive and metabolic effects in the populations where it has been studied longest.
What can actually shift my ovarian aging trajectory?
This is where the audience gets the least honest answer in the consumer market and the most overconfident one in the supplement space. The evidence for DHEA (dehydroepiandrosterone, an adrenal steroid hormone) and CoQ10 (coenzyme Q10, a mitochondrial cofactor) in raising AMH is largely from small RCTs in women with diminished ovarian reserve undergoing fertility treatment. A 2023 network meta-analysis suggests a modest AMH increase (standardized mean difference around 0.35) in that specific population. The effect in healthy non-infertile women is not established. The effect on live birth in healthy women is not established. “Reverse ovarian aging” is over-extrapolation.
What the research supports as legitimate leverage over ovarian and cardiometabolic aging together: do not smoke, address chronic stress and sleep loss seriously, train against resistance two to three times per week, maintain visceral adiposity in a healthy range, address insulin resistance early using markers like HOMA-IR (homeostatic model assessment of insulin resistance, a calculation from fasting glucose and insulin) and A1c (glycated hemoglobin, a 3-month blood sugar average), and address blood pressure and ApoB at the population threshold rather than waiting for symptoms. None of these will turn back the primordial follicle clock. All of them act on the shared aging biology the AMH trajectory is partly reflecting.
The aspirational longevity story is the drug pipeline. The practical longevity story is sleep, strength, glucose, ApoB, blood pressure, and the relationships and meaning that make a long life worth living. Both can be true.
The short version: the protocols sold to raise AMH have small evidence in the wrong population for healthy women, and the leverage you actually have over ovarian and cardiovascular aging is in the unglamorous foundation work.
What I’d do this week
If you have already ordered an AMH test or are about to, read the decision card below before any next step. The card is doctor-grade education, not a substitute for working with your own clinician.
The AMH Decision Card
The four questions to ask your doctor (if you already have a result):
1. Was I on hormonal contraception when this was drawn, and if so, what is the interpretation given that AMH is suppressed about 24% by combined oral contraceptives?
2. What is my AMH in the context of my chronological age, not just an absolute number?
3. Does this result change any clinical decision I am actually making right now, or is it information without a next step?
4. Given that low AMH in women under 44 did not lower natural conception odds in the Steiner 2017 JAMA study, what does this number actually tell me about my fertility timeline?
Caveat row: This card is education for healthy women considering ovarian age testing. It is not a substitute for individualized care with a reproductive endocrinologist or your primary clinician. If you have a known fertility diagnosis, oncologic history, or suspected POI, the conversation is different.
The hardest part of the AMH conversation is not interpreting the number, it is sitting with a woman who just learned a result she was not prepared to receive and helping her see that the number is information, not a verdict
So what should I actually take away from this?
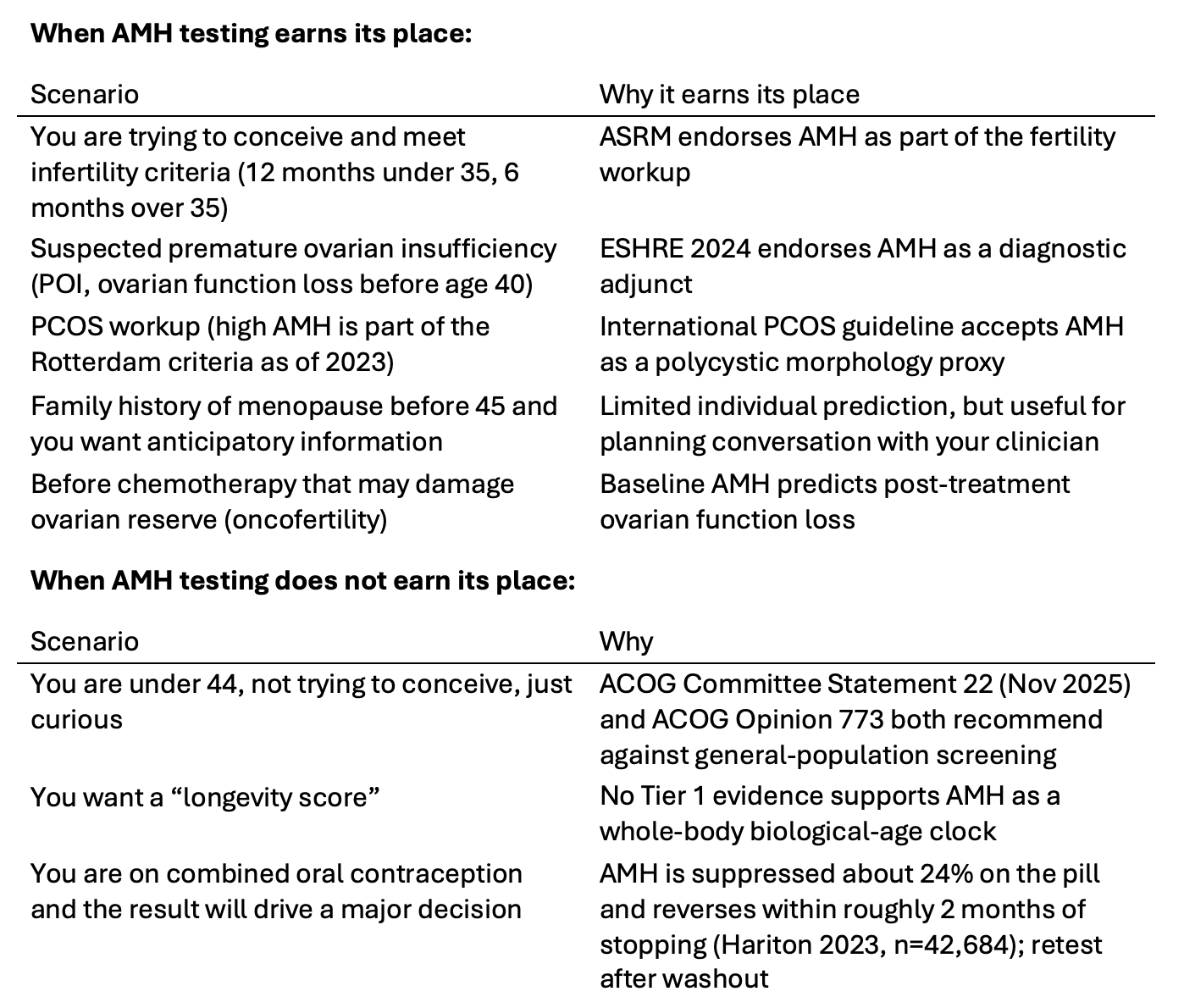
Here is the way I hold this clinically. AMH is the best blood marker of ovarian reserve currently available, and it earns its place inside a specific set of clinical scenarios: infertility workup, suspected premature ovarian insufficiency, PCOS diagnosis, oncofertility planning, and anticipatory conversations when there is a family history of early menopause. Outside those contexts, the population-level evidence does not support general screening. The cardiometabolic signal in faster AMH decline is real and the trajectory is worth knowing, but the leverage that actually moves cardiovascular outcomes for a woman in her thirties or forties lives in sleep, strength, blood pressure, ApoB, glucose handling, and visceral adiposity, not in the number itself. The “ovaries are the master clock” framing is industry narrative running ahead of Tier 1 evidence. The longevity drug pipeline is genuinely interesting and is not yet a recommendation.
The number on your AMH report is information. It is not a verdict. What you do with the rest of your physiology matters more than the value on the page.
I built Blue Yarrow because I want to share my naturopathic doctor training and knowledge so that people who are not getting answers from conventional doctors can find the answers with me. If you bookmark this post and return to it the next time someone in your life forwards you a femtech ad or a longevity-drug headline, that is exactly the use I built it for.
Frequently asked questions
Is AMH the same as my egg count? No. AMH is produced by the small growing follicles inside the ovary at any given moment. Your total reserve of dormant eggs (the primordial follicle pool) is not directly measured by any blood test currently available in clinical use. The “egg count” framing is marketing shorthand, not biology, and reading the test result with that mental model leads to misinterpretation.
Can a low AMH at 33 mean I am about to enter menopause? Almost never. The Depmann 2018 meta-analysis showed AMH adds only 2 percentage points of predictive accuracy over age alone for menopause timing, and the prediction interval for any individual woman in her early thirties is too wide to plan around. The strongest menopause prediction comes only at very low AMH on an ultrasensitive assay in women already 42 or older.
If my AMH is low, should I freeze my eggs? The Steiner 2017 JAMA study showed low AMH in women under 44 did not lower natural conception odds, and ACOG and ASRM do not endorse AMH-driven egg-freezing in women without a fertility diagnosis. Egg-freezing decisions are personal and involve the full picture of family planning, partner status, finances, and ovarian-response prediction with a reproductive endocrinologist. AMH alone should not drive that decision.
Does birth control affect my AMH result? Yes, in a meaningful way. Combined oral contraceptive use is associated with about 24% lower AMH in a study of 42,684 women (Hariton 2023). The effect fully reverses within roughly two months of stopping the pill. If your AMH was drawn on hormonal contraception and the result is driving a major decision, retesting after washout is the most honest read.
Is AMH a longevity score or a biological-age clock? There is no Tier 1 evidence supporting AMH as a whole-body biological-age clock. There is a real population-level signal that faster AMH decline tracks higher cardiovascular disease incidence over twenty years (de Kat 2017, Doetinchem n=3,108), but the causal direction is unresolved and the signal is concentrated in a single cohort. AMH is a reason to take ovarian-age data seriously at the population level, not a personal longevity verdict.
Should I take supplements like DHEA or CoQ10 to raise my AMH? The evidence for DHEA and CoQ10 raising AMH comes from small RCTs in women with diminished ovarian reserve undergoing fertility treatment, where the effect is modest. The effect in healthy non-infertile women is not established, and “reverse ovarian aging” is over-extrapolation. The leverage that matters most over both ovarian and cardiovascular aging is the foundation work of sleep, strength training, blood pressure, ApoB, glucose handling, and stress.
This content is for educational purposes only and is not medical advice. Please consult with your healthcare provider for individual recommendations.
References
1. American College of Obstetricians and Gynecologists. (2019). Committee Opinion No. 773: The use of antimullerian hormone in women not seeking fertility care. Obstetrics and Gynecology, 133(4), e274-e278. PMID: 30913192. https://doi.org/10.1097/AOG.0000000000003162
2. American College of Obstetricians and Gynecologists. (2025, November). Committee Statement No. 22: Anticipatory counseling regarding ovarian-factor fertility decline. Obstetrics and Gynecology. https://www.acog.org/clinical/clinical-guidance/committee-statement
3. de Kat, A. C., Verschuren, W. M., Eijkemans, M. J. C., Broekmans, F. J. M., and van der Schouw, Y. T. (2017). Anti-Mullerian hormone trajectories are associated with cardiovascular disease in women: results from the Doetinchem cohort study. Circulation, 135(6), 556-565. https://doi.org/10.1161/CIRCULATIONAHA.116.025968
4. Depmann, M., Eijkemans, M. J. C., Broer, S. L., Tehrani, F. R., Solaymani-Dodaran, M., Azizi, F., et al. (2018). Does AMH relate to timing of menopause? Results of an individual patient data meta-analysis. Journal of Clinical Endocrinology and Metabolism, 103(10), 3593-3600. https://doi.org/10.1210/jc.2018-00724
5. Finkelstein, J. S., Lee, H., Karlamangla, A., Neer, R. M., Sluss, P. M., Burnett-Bowie, S. M., et al. (2020). Antimullerian hormone and impending menopause in late reproductive age: the Study of Women’s Health Across the Nation. Journal of Clinical Endocrinology and Metabolism, 105(4), e1862-e1871. https://doi.org/10.1210/clinem/dgz283
6. Hariton, E., Shirazi, T. N., Douglas, N. C., Hershlag, A., and Briggs, S. F. (2023). Contraceptive-specific antimullerian hormone values in reproductive-age women: a population study of 42,684 women. Fertility and Sterility, 119(5), 791-799. https://doi.org/10.1016/j.fertnstert.2023.01.024
7. Iwase, A., Hasegawa, Y., Tsukui, Y., Kobayashi, M., Hiraishi, H., Nakazato, T., and Kitahara, Y. (2024). Anti-Mullerian hormone for screening, diagnosis, evaluation, and prediction: a systematic review and expert opinions. Journal of Obstetrics and Gynaecology Research, 50(1), 15-31. https://doi.org/10.1111/jog.15818
8. Practice Committee of the American Society for Reproductive Medicine. (2020). Testing and interpreting measures of ovarian reserve: a committee opinion. Fertility and Sterility, 114(6), 1151-1157. https://doi.org/10.1016/j.fertnstert.2020.09.134
9. Steiner, A. Z., Pritchard, D., Stanczyk, F. Z., Kesner, J. S., Meadows, J. W., Herring, A. H., and Baird, D. D. (2017). Association between biomarkers of ovarian reserve and infertility among older women of reproductive age. JAMA, 318(14), 1367-1376. https://doi.org/10.1001/jama.2017.14588